
Annular Tear
What Is an Intervertebral Disc?
The intervertebral disc is a fibrocartilaginous structure located between adjacent vertebral bodies in the spine. Each disc serves as a shock absorber, allows flexibility, and helps maintain proper spacing and alignment of the vertebrae.
The adult human spine typically has 23 intervertebral discs—6 in the cervical region, 12 in the thoracic region, and 5 in the lumbar region. There are no discs between the occiput and C1 or between C1 and C2, and none in the sacrum or coccyx, as these are fused segments.
Structure of the Disc
Each disc consists of two main components:
- Nucleus Pulposus: A gel-like core rich in proteoglycans and water, allowing it to absorb compressive forces.
- Annulus Fibrosus: A tough, multi-layered outer ring made of type I collagen that provides tensile strength and protects the nucleus pulposus.
Function and Natural Degeneration
The disc enables movement such as flexion, extension, and rotation. Over time, the disc undergoes normal wear and tear—a process called disc degeneration. This may include dehydration of the nucleus, thinning of the annulus, and loss of disc height, often leading to conditions like bulging discs or tears.
Pathological Annular Tears
Annular tear or annular fissure or simply disc tear is a deficiency of one or more layers of the annulus fibrosus. While some annular fissures may occur as part of natural aging, others are considered pathological when associated with symptoms such as axial or radicular pain. Pathological tears can allow disc material to escape or provoke inflammation by exposing nerve endings to the inner nucleus.
Most disc tears are asymptomatic, but some may be painful. Typically, simple symptomatic annular fissures without disc herniation are treated with non-steroidal anti-inflammatory medications and low-impact physical therapy. Chronic pain due to disc tears can be due to granulation tissue or in-growth of nerve endings which is usually seen near the dorsal root ganglion. Additionally, a disc tear can allow extrusion, for example, disc herniation, of the nucleus pulposus and compress the adjacent nerves.
Modified Dallas Classification
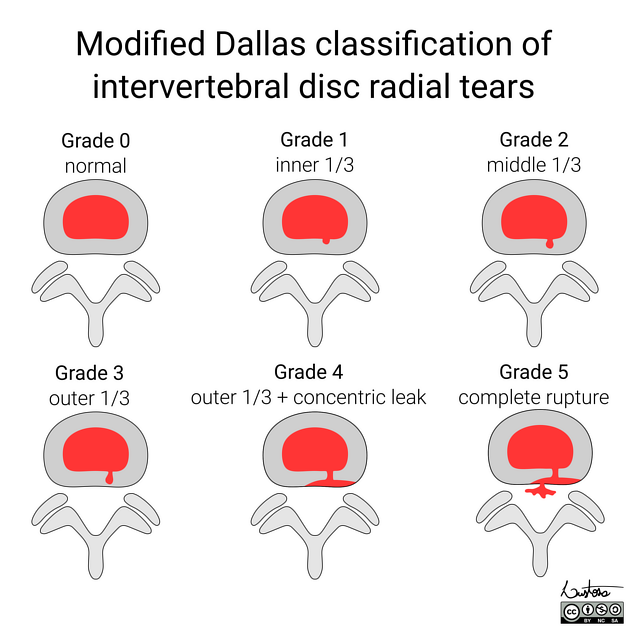
The Modified Dallas Classification is a grading system used to describe the extent of annular fissures seen on MRI or discography:
- Grade 0: No annular tear or fissure.
- Grade 1: Tear extending to the inner one-third of the annulus.
- Grade 2: Tear reaching the middle third of the annulus.
- Grade 3: Tear reaching the outer third of the annulus.
- Grade 4: Tear reaching the outer third with contrast tracking radially outward.
This classification helps in evaluating the severity of disc injury and guides treatment planning.
Etiology
The annulus fibrosus is the type I collagen surrounding the nucleus pulposus in approximately 15-20 layers. Together, the annulus fibrosis and nucleus pulposus form the intervertebral disc between adjacent vertebrae. The annulus fibrosus runs obliquely between edges of adjacent vertebrae, connecting the inferior endplate of the superior vertebra with the superior endplate of the inferior vertebra. The directions of the layers of the annulus fibrosus alternate which adds to the strength of the annulus fibrosus. Near the central region, the annulus fibrosus blends with the nucleus pulposus. The posterolateral aspect of the annulus fibrosus has a greater content of vertically oriented fibers leading to relative focal weakness at the posterolateral aspect. This anatomy of the annulus fibrosus explains why most annular fissures are at the posterior or posterolateral aspect of the annulus fibrosus.
Epidemiology
Annular or disc tears are commonly identified in asymptomatic individuals during imaging for other reasons. Estimates for annular tears in adults range from a few precents to upward of 50% depending on the criteria and imaging used to identify an annular tear.
Pathophysiology
The posterolateral aspect of the annulus fibrosus has a greater content of vertically oriented collagen fibers. In other regions of the annulus fibrosus layers are alternating obliquely oriented layers. Thus in the postero-lateral region, the vertical alignment of the fibers is more likely to allow for focal deficits of the annulus fibrosus and tearing or separation between the vertically oriented fibers.
History and Physical
Most annular fissures or annular tears are asymptomatic and discovered incidentally on imaging. If an annular fissure or tear is symptomatic, it may cause one of two findings: localized pain secondary to the tear or radicular symptoms secondary to irritation of the passing nerve root. The pain may either be acute if the tear occurs suddenly or more chronic if there is a slower development of the annular fissure.
If the annular fissure is locally symptomatic, it may cause pain localized deep pain worse with movements that can stress or irritate the focal annular tear. In such cases, there is no radicular nerve involvement, and the physical exam may be unrevealing. Sometimes the annular tear can irritate the traversing nerve and cause radiculopathy. If the annular fissure or annular tear is significant enough, disc material can herniate to irritate or compress traversing nerves or spinal cord. In either case, when the traversing nerve is irritated, it can cause radicular symptoms including pain, paresthesia, and/or weakness depending on the extent of nerve irritation or compromise.
Evaluation
An annular fissure can be concentric, transverse, or radial in orientation and may involve some or all layers. On magnetic resonance imaging (MRI) T2 sequence, the annular fissure is hyperintense (bright) compared to the rest of the annulus fibrosus (which is normally hypointense or dark) due to the relative increase in water content at the fissure compared to the normal annulus fibrosus.
If there is herniation of intravertebral disc material, there must be incompetence of the annulus fibrosus, and thus, an annular fissure or annular tear must be present even if not specifically visualized on the imaging. Thus, an annular fissure or annular tear can be implicated any time intravertebral disc herniation is identified.
If you are unable to have an MRI, a computed tomogram (CT) myelogram may show nerve root or cord compression from a disc protrusion. The CT scan can not identify the edema of an annulus fibrosus tear or fissure and thus, it is less sensitive than MRI.
Treatment / Management
An annular fissure or tear can be symptomatic or asymptomatic. Symptomatic annular fissures can occur with or without intravertebral disc protrusion or herniation. Each entity is discussed separately below.
Asymptomatic Annular Tear
If the annular fissure is identified incidentally, most commonly on MRI imaging, then no treatment is warranted. Such annular fissures may resolve spontaneously over time and are frequently due to the stresses applied to the spine. It is posited that some asymptomatic annular fissures may become symptomatic with time, but there is currently no definitive evidence that the treatment of asymptomatic annular fissures provides any benefit or prevents any future issues.
Symptomatic Annular Tear without Disc Protrusion or Herniation
An annular fissure or tear can be symptomatic without disc protrusion or herniation. It is suspected that local inflammatory reactions from the annulus fibrosus tear or fissure lead to irritation of adjacent nerve fibers or traversing nerve roots. The mainstay of treatment for such situations is non-steroidal anti-inflammatory medications as well as low-impact physical therapy. The non-steroidal anti-inflammatory medications may help decrease the inflammatory reaction at the annular fissure which decreases stimulation or irritation of adjacent nerve fibers or traversing nerve roots. The low-impact physical therapy may help strengthen core muscles to mitigate the forces which may have originally led to the annular fissure or tear. Some have suggested local transforaminal steroid injections may alleviate the symptoms more quickly.
Some have argued that long-standing annular fissures or tears may lead to granulation tissue formation at the site of the annulus fibrosus tear or fissure. This local granulation tissue can either irritate or compress the traversing nerve root and lead to a radicular pattern of symptoms. The first-line treatment for such situations is non-steroidal anti-inflammatory medications and low impact physical therapy as discussed above with or without transforaminal steroid injection. In longer-standing cases or instances with weakness or progression some suggest decompression of the nerve with a foraminotomy may prevent further deterioration and improve the symptoms. Some have suggested resecting the granulation tissue itself.
Symptomatic Annular Tear with Disc Protrusion or Herniation
If there is disc protrusion or herniation, it is usually the protruding or herniated disc material itself which causes the clinical symptoms. In such cases, the patient is treated for the disc protrusion or herniation and not the annular fissure or tear. Treatment options for disc protrusion or herniation including conservative measures of nonsteroidal anti-inflammatory medications, physical therapy, and local injections. If symptoms fail to improve, symptoms progress or the patient develops weakness surgical treatment options should be considered including laminotomy, laminectomy, foraminotomy, discectomy, fusion, or some combination thereof. If a discectomy is performed there has been no convincing evidence that closure of the annular fissure, tear, or annulotomy significantly affects the long-term outcome for the patient.
Discography: Rise, Utility, and Decline
The discogram was once widely used to identify painful discs by injecting contrast into the disc and reproducing concordant pain. It was especially used in surgical planning. However, multiple studies—including a notable prospective study published in Spine Journal (Carragee et al., 2009)—demonstrated a high false-positive rate and the potential for accelerating disc degeneration in otherwise non-pathologic discs. As MRI improved in sensitivity, discography declined in clinical utility and is now rarely used, often reserved for complex preoperative cases.
Intradiscal Procedures: IDET, Biacuplasty, and More
To address pain from annular fissures, several intradiscal procedures have emerged:
- Intradiscal Electrothermal Therapy (IDET): Uses heat via a catheter to denature pain fibers and shrink collagen. Mixed evidence—initial enthusiasm has waned.
- Biacuplasty: Utilizes bipolar radiofrequency to deliver controlled heat to the posterior annulus. Shown to reduce pain in select patients with discogenic low back pain (Kapural et al., Pain Med. 2013).
- Annulo-nucleoplasty: Combines mechanical decompression with thermal coagulation of disc tissue. Often used when small herniations are involved.
While results vary, these procedures may be considered in well-selected patients who fail conservative care and have MRI evidence of high-intensity zones (HIZ) suggestive of annular tears.
Disc-FX Procedure: Mechanism and Clinical Use
Disc-FX is a minimally invasive intradiscal procedure designed to treat contained discogenic back pain and small annular tears. It combines nucleus ablation, annuloplasty, and nucleus modulation using radiofrequency energy delivered through a percutaneous access cannula.
The procedure typically uses a small access tube placed through Kambin’s triangle under fluoroscopic guidance. A bipolar radiofrequency probe (such as Trigger-Flex) is then used to ablate nociceptive fibers in the annulus fibrosus, shrink collagen in the annular wall, and decompress the nucleus pulposus through evaporative ablation.
Scientific rationale: Studies show that annular fissures may house nociceptors and inflammatory mediators contributing to chronic pain. Disc-FX targets these structures while preserving disc height and avoiding open surgery. It is typically performed under conscious sedation in an outpatient setting.
Clinical Indications: Disc-FX is best suited for patients with:
- Contained disc herniations (not sequestered)
- Discogenic pain confirmed via MRI and/or provocative discography
- Annular fissures with or without high-intensity zones (HIZ)
- Failure of conservative therapy
Initial outcome studies and case series suggest that Disc-FX offers pain reduction and functional improvement in select patients with discogenic low back pain. Long-term data and randomized controlled trials are still limited.
Disc-FX represents a modern evolution of intradiscal therapy, offering a bridge between conservative care and more invasive spinal surgery.
Regenerative Medicine for Annular Tears
Emerging treatments involve biologic injections into the disc to promote healing and reduce inflammation. These include:
- Platelet-Rich Plasma (PRP): Autologous platelets injected into the disc may reduce pain by releasing anti-inflammatory cytokines. Small trials like Tuakli-Wosornu et al. (PM&R, 2016) report reduced pain scores at one year.
- Stem Cell Therapy: Bone marrow-derived mesenchymal stem cells (BMSCs) may aid in disc matrix repair. Though still investigational, preliminary results show promise in select patients (Amirdelfan et al., Stem Cells Int. 2019).
Prognosis
The natural history of mechanical back pain due to annular tears is typically benign. Most patients experience improvement over time with conservative care. Surgical intervention is generally reserved for cases with neurologic deficit or unrelenting pain despite other interventions.
Dr. Amit Sharma & our minimally invasive pain & spine team.
Key References
- Amirdelfan K, et al. Transforaminal Intradiscal Injection of Bone Marrow Aspirate Concentrate for Discogenic Pain. Stem Cells Int. 2019. PubMed
- Kapural L, et al. Radiofrequency Bipolar Annuloplasty for Discogenic Pain: Biacuplasty. Pain Med. 2013. PubMed
- Tuakli-Wosornu YA, et al. PRP for Lumbar Disc Pain. PM&R. 2016. PubMed
- Carragee EJ, et al. Are Lumbar Disc Injections Harmful? Spine J. 2009. PubMed
- StatPearls; authors: Steven Tenny, Christopher C. Gillis.
- Hacking C, Sharma R, Modified Dallas discographic classification of intervertebral disc radial tears. Reference article, Radiopaedia.org (Accessed on 09 May 2025) https://doi.org/10.53347/rID-191354.



