
Back Pain: How Spine Specialists Diagnose the Real Cause
Most back pain is not diagnosed by MRI alone. The key is matching the pain pattern, physical examination, and imaging findings to identify the structure actually causing symptoms. This guide explains how spine specialists approach that process.
 John is a 45-year-young gentleman. He has served many years as a firefighter, saving lives. He had an episode of severe back pain in his 20s while playing lacrosse. That injury left him bedridden for a few days. He saw a chiropractor back then and was up and running in no time. His job and two kids keep him moving day in and day out.
John is a 45-year-young gentleman. He has served many years as a firefighter, saving lives. He had an episode of severe back pain in his 20s while playing lacrosse. That injury left him bedridden for a few days. He saw a chiropractor back then and was up and running in no time. His job and two kids keep him moving day in and day out.
In June 2020, John was lifting a heavy piece of furniture with a friend when he felt a small “pop” in his lower back. He did not think much of it. He woke up with severe back stiffness the next morning.
COVID-related restrictions were still ongoing. He avoided his family doctor, and his old chiropractor was not seeing patients either. He iced his back for a few days, but the spasms would not resolve. After a week of suffering, he ended up at an urgent care facility, where he was seen briefly.
The on-site X-ray was read as “normal.” He was given prescription-grade ibuprofen and a muscle relaxer, and reassured that he would feel better soon.
Before John’s story continues, it helps to refresh the basics of the nervous system and spine anatomy.
Introduction
Spine pain — neck, mid-back, or low back — needs little introduction. It is the leading cause of disability worldwide, and the published literature on it is vast. A simple search returns enough material to review for weeks. For figures and statistics, the Statista back pain report is a useful reference.
Three numbers put the scale in perspective:
39%
OF US ADULTS EXPERIENCED BACK PAIN IN THE LAST 3 MONTHS
54%
OF US ADULTS HAD NECK OR BACK PAIN FOR 5 YEARS OR LONGER
73%
OF US ADULTS TOOK NSAIDS LIKE IBUPROFEN FOR NECK OR BACK PAIN
The purpose of this guide is not to add to that pile, but to explain how spine specialists actually approach the problem. The term “back pain” is used throughout, since low back pain is more common than neck pain, but the same fundamentals apply to both.
The spine is a complex structure of interconnecting bones, ligaments, muscles, joints, and cartilage — all working together to provide support, strength, and flexibility. It also sheathes the spinal cord and nerve roots, the cable connecting the body to the brain. This complexity leaves the spine susceptible to injury and pain, and pain from one or more of these structures often presents in remarkably similar ways. Back pain is a puzzle to solve from the outset.
Know the Basics
Back pain affects people of all ages. It takes a toll on personal life and remains a leading cause of lost productivity at work. Before learning how doctors approach back pain, it helps to understand the spine itself — it makes the sections that follow far easier to follow.
What’s Your Problem?
Many clinicians are not drawn to solving the back pain riddle. A long-standing belief holds that more than 90% of acute back pain patients improve over time, with or without aggressive treatment, and symptoms are often downplayed early on because of it. That conviction stems from older research. More recent work examining the natural course of back pain concludes that it is not a self-limiting problem, but rather a recurrent and sometimes persistent disorder.[1], [2], [3], [4], [5], [6]
Most low back pain episodes are short-lived, at least in the primary care setting. In the long term, however, low back pain often runs a persistent course, with roughly two-thirds of patients estimated to still have pain at 12 months. Some people never experience low back pain, but most have it on and off, or persistently. At the first visit for new-onset back pain, the eventual trajectory is hard to predict.
The picture grows more complex once you know that many people with real structural findings — disc bulges, herniations or tears, spinal arthritis, minor fractures, benign tumors — never feel back pain at all. Diagnosing the *cause* of back pain is therefore not easy. It demands attention to detail, a thorough examination, and the right tests (X-ray, CT, or MRI) for the individual.
The process may require treatment trials — core strengthening with a physical therapist, traction with a chiropractor — or a course of oral anti-inflammatories or muscle relaxers, or targeted spinal injections of local anesthetic or corticosteroid. The response to each step adds information that helps narrow toward a specific diagnosis.
Where to Start?
By the time you are reading this, you or your suffering loved one may have already seen several doctors — a primary physician, an urgent care, perhaps an emergency department. Do not be discouraged if you were not taken “seriously.” Because most people improve after an initial severe episode, it is natural for the first visit to be downplayed. Once that first episode fails to resolve, or grows into a larger and more persistent problem, it is time to take the pain more seriously and see a spine specialist.
Spine and back pain specialists come from diverse backgrounds and view spinal problems differently. A physical therapist’s or acupuncturist’s approach differs from a chiropractor’s; a spine interventionalist has different objectives than a spine surgeon. It is worth seeking more than one expert opinion and learning as much as possible.
At SpinePain Solutions, we work closely with your physical therapist or chiropractor to formulate a minimally invasive, tailored treatment plan. Our pain physicians and spine surgeons collaborate on each case, guided by a single core principle: superior patient outcomes.
Approach to Spine Pain
With the basics of spine structure in hand, and an understanding of the challenges clinicians face, a simple approach to spine pain comes into view. A few questions guide it:
- Is the pain recent, a pattern of episodic pain, or a chronic and progressively declining condition? (Apples & Oranges)
- Do the symptoms match the structural changes seen on MRI? (Pieces of the Puzzle)
- Is the pain axial, radicular, or mixed? (The Big Three)
- Is there a need for spine diagnostics to identify the source? (The Culprit)
- Are there red flags that warrant further testing or additional specialists?
Red Flags for Back Pain
History — what your doctor may ask:
- Cancer
- Unexplained weight loss
- Immunosuppression
- Prolonged steroid use
- Intravenous drug use
- Urinary tract infection
- Pain that is increased, or unrelieved, by rest
- Fever
- Trauma significant for the patient’s age (a fall from height or motor vehicle accident in a younger person; a minor fall or heavy lift in an older or potentially osteoporotic person)
- Bladder or bowel incontinence
- Urinary retention with overflow incontinence
Physical signs — what your doctor may find on examination:
- Fever
- Saddle anesthesia
- Loss of anal sphincter tone
- Major motor weakness in the lower extremities
- Vertebral tenderness
- Limited spinal range of motion
- Neurologic findings persisting beyond one month
Apples & Oranges
Once red flags are ruled out, the first thing most spine specialists assess is the onset and pattern of the pain. It matters whether the problem is acute (recent), a pattern of episodic pain, or a chronic and progressively declining condition.
No two back pain patients are the same, and no two episodes in the same person can be assumed identical. A fall off a skateboard as a teenager may have caused a first episode, but a heavy lift a decade later is probably not the same pain. Although an acute episode can be the start of a problem that eventually becomes episodic or chronic, it is investigated and treated differently at the outset.



Teenagers frequently present with neck or back pain from muscle sprains, minor injuries to spinal ligaments or facet joints, and occasionally benign stress fractures (spondylolysis). Younger adults are often injured in traffic accidents or workplace falls, leading to soft-tissue injuries, minor disc tears (annular fissures), disc herniations, or facet joint injuries.
Patients in their golden years more often present with degenerative conditions — osteoporotic compression fractures, facet joint arthritis, degenerative disc disease, or spinal stenosis. Age is not a strict criterion, only an indicator: plenty of younger people have degenerative findings, and many seniors have simple sprains or minor disc issues.
Pieces of the Puzzle
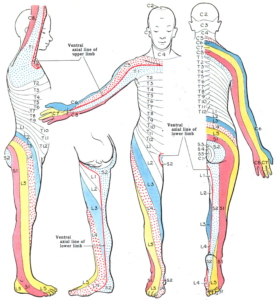
Consider a more specific case. Pain that radiates from the lower back into the outer thigh (between hip and knee), crosses below the knee to the outer lower leg, and travels to the top of the foot and big toe is called radicular pain in an L5 distribution — the area supplied by the L5 nerve root (shaded yellow on the dermatome map).
When the L5 nerve root is pinched, the muscle most likely to weaken is the extensor hallucis longus (EHL), which lifts the big toe. Reflex changes are variable at L5. When the pain pattern, the EHL weakness, and a matching MRI finding all line up, the diagnosis of L5 radiculopathy becomes firm. This triad returns in John’s case below.
It is worth emphasizing that clean, textbook cases like this are not the norm. For reference, the dermatomes (skin supplied by a single nerve root), myotomes (muscles supplied by one nerve root), and corresponding reflex changes are outlined here.


One of the recurring challenges in the spine world is the lack of consistent findings needed to reach a conclusive diagnosis. A patient with a clear history of a pinched left L3 nerve may show no matching neurologic findings; when symptoms and exam do correlate, the MRI may show a herniation on the opposite side or at an unexpected level. Solving these cases is what makes the work interesting.
Patients are given ample time to describe their pain. They are examined directly, and the MRI films are reviewed personally rather than relying solely on an outside report. These pieces of information are vital to solving the underlying problem. When a case is perplexing, more minds are brought in during the same visit — and there is no shame in asking a colleague for a second look.
Based on the initial assessment, a doctor may order X-rays, CT, or MRI. Each provides different information.
X-rays [7]
X-rays (radiographs) are the most common and widely available imaging technique. They take seconds, rarely require insurance authorization, and show bony structures — alignment and the health of the spinal bones — well enough to rule out major fractures. Soft tissues (muscles, ligaments, discs, nerves) are not visible, but some can be inferred: narrowing between two vertebrae suggests a degenerated or herniated disc, and degenerative changes in the adjacent bone make a degenerative disc more likely. A lumbar spine X-ray delivers roughly 1.5 mSv.









CT Scan (Computed Tomography)
CT combines X-rays with computer processing to produce detailed cross-sectional images. It is far more sophisticated than plain film, takes several minutes, and delivers more radiation — a lumbar CT is roughly 6 mSv. CT excels at bony detail but gives limited soft-tissue information. It usually requires insurance authorization, and for patients with implanted metal devices in whom MRI is contraindicated, CT may be the only option. The radiation from a single CT scan is very unlikely to cause meaningful harm; the relevant concern is cumulative dose across many repeat scans over a lifetime.
MRI Scan (Magnetic Resonance Imaging)
MRI produces cross-sectional images without ionizing radiation, using magnetic fields and computer processing to capture high-resolution pictures of bone and soft tissue. It may not be possible with a pacemaker, certain implants, metal clips, or other metal objects. MRI is the gold standard for the spine: less detailed on bone than CT, but far superior for soft tissues — ligaments, discs, spinal cord, and nerves. It usually requires insurance authorization.
Once imaging is available, the specialist puts the pieces together into an initial diagnosis. This part is challenging but essential. Nearly a third of healthy people with no pain at all have a degenerated or herniated disc, or other positive findings, on CT or MRI. The goal is to match the reported pain, the physical exam, and the imaging. When all three align, the case is rarely disputed between experts, and recommendations from different specialists tend to agree.
The Big Three
Axial Pain
- Pain mostly around the core: neck, mid-back, or low back.
- May radiate to the shoulder (from the neck), the flank (from the mid-back), or the buttocks and hips (from the low back).
- Common causes include degenerative disc disease, vertebrogenic pain from Modic endplate changes, annular tears, facet joint injury or arthritis, sacroiliac joint issues, or muscle sprains.
Radicular Pain
- Pain predominantly radiating down an arm, around the chest wall to the belly or groin, or down a leg.
- Common causes include herniated discs, foraminal or central spinal stenosis, or piriformis syndrome.
Mixed Pain
- Pain affecting the core and carrying a radicular or non-radicular component.
- The most common of the three.
- Causes span the full list of spine conditions outlined below.
The Culprit
Once the pieces are gathered, a preliminary diagnosis takes shape — the cause of the pain, the real culprit. Most of the time it can be made from the pain description, the exam, and the MRI. When those pieces do not add up cleanly, spine diagnostics help.
Spine diagnostics is an area of interventional pain medicine in which small doses of a local anesthetic, sometimes with corticosteroid, are placed at designated targets to confirm a diagnosis. These test injections carry a risk of false-positive and false-negative responses, but combined with imaging they improve diagnostic accuracy. They must be performed in a controlled fashion by a trained, experienced physician. EMG and nerve conduction studies, performed by a neurologist, are another diagnostic modality.
Cases
With the framework in place, John’s story shows it in action.
John’s story is worth following in full, because over five years he developed two completely different spine problems — one radicular, one axial — and each demanded its own workup. He is the whole framework in a single patient.
Chapter 1 — Radicular Pain: The Herniated Disc (2020)
When we last left John, he had hurt his back lifting heavy furniture and been sent home from urgent care with ibuprofen and a muscle relaxer. His misery did not end there. Four days later he returned, now with pain radiating into his left leg — buttock, outer thigh, down the calf, to the top of the left foot.
At that visit he was told he had “sciatica,” given a steroid pack, and referred to physical therapy. Within two days of the steroids his back and leg felt better. He started PT, but within a week the pain returned with a vengeance — the sciatica was worse, and his left leg now felt numb. Frightened of losing his livelihood, or worse, he called his family doctor and was urgently referred to our center.
 John was seen in late July. Red flags were ruled out first. On examination, there was numbness in the left L5 dermatome — the same distribution set up earlier in this guide. This is where the L5 triad pays off: the pain pattern was textbook L5, and the next thing to check was the extensor hallucis longus. John’s strength was preserved; he favored the left leg from pain but could walk with discomfort. He went for MRI the same day.
John was seen in late July. Red flags were ruled out first. On examination, there was numbness in the left L5 dermatome — the same distribution set up earlier in this guide. This is where the L5 triad pays off: the pain pattern was textbook L5, and the next thing to check was the extensor hallucis longus. John’s strength was preserved; he favored the left leg from pain but could walk with discomfort. He went for MRI the same day.
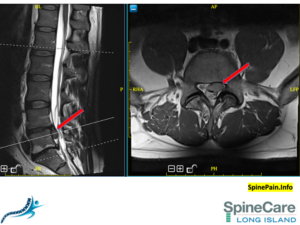
The films showed a large extruded disc herniation on the left (red arrows), compressing the L5 nerve root — matching the pain and the exam. A formal diagnosis of lumbar radiculopathy from a herniated disc was made. The pieces fit: pain pattern + dermatome + imaging, all pointing to the same nerve root.
John underwent a selective nerve root block, which served two purposes: it confirmed the L5 root as the pain generator and gave him real relief, becoming pain-free within a week. He returned to physical therapy for core strengthening. For several months he did well — but the relief did not hold. The leg pain returned, and a repeat MRI showed a persistent large extrusion at the same level. Having exhausted reasonable conservative care for a structurally confirmed, symptomatic herniation, John was a clear candidate for definitive decompression.
Rather than a traditional open microdiscectomy, John underwent an endoscopic discectomy — a minimally invasive procedure in which the herniated fragment is removed through a small portal under direct camera visualization, sparing the surrounding muscle and bone. He recovered quickly, the leg pain resolved, and as a firefighter he was back to full duty with minimal downtime. His L5 radiculopathy was, at last, definitively solved.
Chapter 2 — Axial Pain Five Years Later: The Diagnostic Detective Work (2025)
John did well for five years. Then, at 50, he returned with something that felt entirely different. There was no leg pain this time. Instead, he described a deep, midline ache across his lower back — worst when he sat through a long shift at the firehouse, leaned over paperwork, or drove, and easier when he stood and moved around. This was not his old sciatica. By pattern alone, this was axial pain, not radicular — a different branch of the Big Three.
This is exactly the situation where the workup becomes detective work, because several structures can produce axial low back pain and they mimic one another. Rather than guess, John’s team worked through the differential deliberately.
Step 1 — Facet joints ruled out. Facet-mediated pain typically worsens with standing and arching backward; John’s worsened with sitting and bending, which argued against it. To be sure, he underwent diagnostic medial branch blocks — the small anesthetic injections that test whether the facet joints are the source. His relief was minimal. The facets were not the culprit.
Step 2 — Sacroiliac joint ruled out. SI joint pain usually localizes to the back of the pelvis and worsens with transitions and single-leg loading. John’s pain was midline, not over the pelvis, and his provocative SI maneuvers were unremarkable. A diagnostic sacroiliac joint injection likewise failed to relieve him. The SI joint was not the culprit either.
Step 3 — The endplate identified. With facet and SI sources excluded, attention turned to the disc and vertebral endplate. A new MRI showed no nerve compression, but the endplates above and below a degenerated disc now showed Modic changes — inflammatory signal changes at the bone-disc interface. This is the hallmark of vertebrogenic pain, a distinct and underrecognized source of chronic axial low back pain carried by the basivertebral nerve, which runs into the vertebral body and signals from these inflamed endplates. Now the pieces fit again: a flexion-worsened axial pattern, a negative facet and SI workup, and Modic changes on imaging all converging on one source.
Because John’s pain pattern, his diagnostic injections, and his imaging all aligned on a vertebrogenic source, he was a candidate for basivertebral nerve ablation (BVN) — a minimally invasive, outpatient procedure that quiets that specific nerve. He had it done, and his deep axial back pain improved substantially over the following weeks to months. Two very different problems, five years apart, each solved by the same disciplined process.
Why John’s Two Chapters Matter
John’s journey sits at opposite ends of the Big Three. In 2020 his pain was radicular — a pinched nerve root, confirmed by a matching dermatome and MRI, solved by removing the offending disc fragment. In 2025 his pain was axial — no leg involvement, traced through a stepwise elimination of facet and SI sources to an inflamed endplate, then addressed by ablating the basivertebral nerve. Same patient, same spine, entirely different culprits and entirely different approaches. Most real patients land somewhere in the mixed middle, but the framework never changes: match the pattern, the exam, and the imaging, rule out the mimics, then treat the confirmed source.
Axial: Low Back Pain Without Sciatica
Radicular: Sciatica & Radiculopathy
Full Spine Conditions Index
Spinal Column Conditions
-
- Spondylolisthesis and Spinal Instability
- Spinal Stenosis: Central and Foraminal
- Coccydynia
- Skeletal irregularities
- Scoliosis (a curvature of the spine)
- Lordosis (an exaggerated arch in the lower back)
- Kyphosis (an excessive outward arch of the spine)
- Miscellaneous congenital anomalies of the spine
Spine Bone & Joint Conditions
-
- Vertebrogenic Pain
- Compression Fracture
- Spondylolysis
- Facet Syndrome: Sprain, Fracture, Arthritis
- Spina Bifida: incomplete development of the spinal cord and/or its protective covering, which can cause malformed vertebrae, abnormal sensation, and even paralysis
- Osteoporosis: a progressive loss of bone density and strength that can lead to painful vertebral fractures
- Vertebral Osteomyelitis
Disc Conditions
Spinal Nerve Conditions
Conditions Mimicking Spine Disease
Post-Surgical Conditions
Non-Spine Sources
-
- Kidney stones — sharp pain in the lower back, usually on one side
- Endometriosis — uterine tissue growing outside the uterus
- Fibromyalgia — widespread muscle pain and fatigue
- Tumors — pressing on or destroying the bony spine, cord, or nerves
- Pregnancy — back symptoms almost always resolve after delivery
Frequently Asked Questions
Will my back pain just go away on its own?
Many acute episodes settle within weeks, but back pain is often recurrent. Roughly two-thirds of patients still report some pain at twelve months. A first episode that fails to resolve, or keeps returning, deserves a specific diagnosis rather than repeated reassurance.
Does a normal X-ray mean nothing is wrong?
No. X-rays show bone well but cannot show discs, nerves, or other soft tissues. A “normal” X-ray does not rule out a herniated disc, vertebrogenic pain, or nerve compression — that usually requires MRI.
If my MRI shows a herniated disc, is that definitely the cause of my pain?
Not necessarily. Nearly a third of pain-free people have disc bulges or herniations on imaging. A finding only counts when it matches the pain pattern and the physical exam. Matching all three is the heart of an accurate diagnosis.
What is the difference between axial and radicular pain?
Axial pain stays around the core — the neck, mid-back, or low back. Radicular pain shoots down an arm or leg along a nerve root. Many patients have a mix of both, which is the most common pattern.
What is vertebrogenic pain, and how is it different from a disc problem?
Vertebrogenic pain comes from inflamed vertebral endplates — seen as Modic changes on MRI — and is carried by the basivertebral nerve. It causes deep, midline axial low back pain that worsens with sitting and bending. It is a distinct diagnosis from a herniated disc and has its own targeted treatment.
When should back pain be treated as an emergency?
Seek urgent care for progressive leg weakness, numbness in the saddle region, loss of bladder or bowel control, fever with back pain, or significant trauma. These are red flags that warrant immediate evaluation.
What to Expect Moving Forward
Most people with back pain improve with conservative care. Understanding the likely pattern — axial, radicular, or mixed — guides physical therapy, activity changes, and, when needed, targeted diagnostics and procedures. When pain persists or worsens despite appropriate care, a spine specialist can determine whether further testing or interventional options are appropriate. The throughline of this guide is simple: match the pain, the exam, and the imaging, then treat the confirmed source.
A full discussion of spine pain could go on forever. Our team will give you the time and attention you deserve to diagnose your case and build a treatment plan. Text your name and phone number to 631-310-0000.
Dr. Amit Sharma & our minimally invasive pain & spine team.
References
[1] The course of back pain in primary care. Von Korff M, et al. Spine (Phila Pa 1976). 1996.
[6] Trajectories of low back pain. Axén I, et al. Best Pract Res Clin Rheumatol. 2013.
[7] Courtesy: Radiology Masterclass
[8] Figures from Corbett S. Introduction to Spine Surgery. 1st ed. Stuttgart/New York: Georg Thieme Verlag; 2006.



