Facet Joint Syndrome: Symptoms, Diagnosis & Treatment | Dr. Amit Sharma
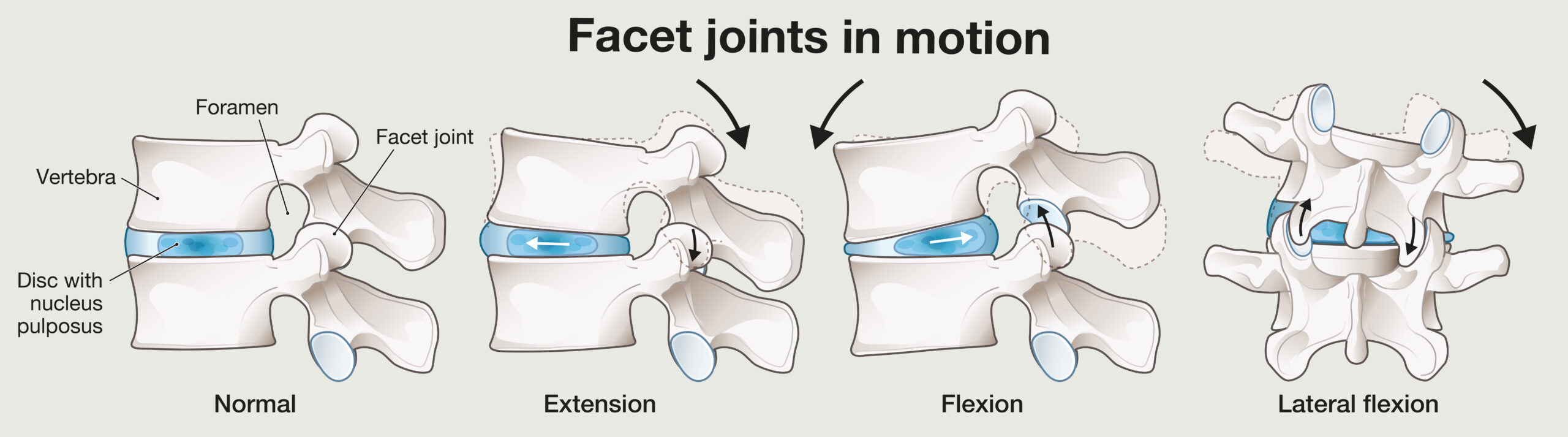
Facet joint syndrome is a common cause of neck pain, back pain, stiffness, and pain that worsens with certain movements. The facet joints are small paired joints in the back part of the spine. They help guide motion, provide stability, and prevent excessive twisting or extension.
When these joints become irritated, arthritic, overloaded, or inflamed, they can become a major pain generator. Facet pain is usually considered axial pain, meaning it tends to stay in the neck, mid-back, or low back region rather than traveling in a classic nerve pattern down the arm or leg.
At our Long Island interventional spine practice, we evaluate facet joint syndrome by combining your symptom pattern, physical examination, imaging, and when appropriate, image-guided diagnostic blocks. This distinction matters because facet pain is treated differently than a herniated disc, sciatica, or cervical radiculopathy.
What Is Facet Joint Syndrome?
Facet joints are located behind the spinal discs. Each joint connects one vertebra to the next. These joints are lined with cartilage and surrounded by a capsule, similar to other joints in the body.
Over time, the cartilage may thin, the joint capsule may become inflamed, and bone spurs may develop. This process is often related to spondylosis, arthritis, repetitive stress, prior injury, disc degeneration, or instability.
Facet joint syndrome does not always mean severe arthritis. Some patients have significant imaging findings with little pain, while others have severe pain from joints that look only mildly abnormal. This is why diagnosis requires more than looking at an MRI alone.
Cervical vs Lumbar Facet Joint Syndrome
Facet joint syndrome can affect different regions of the spine. The symptoms often depend on whether the irritated joints are in the neck, mid-back, or lower back.
Cervical Facet Joint Syndrome
When facet joints in the neck become painful, patients may experience stiffness, aching, pain with turning the head, pain at the base of the skull, headaches, or discomfort traveling into the trapezius or shoulder blade region.
Cervical facet pain often overlaps with neck pain and cervicogenic headache. It is different from cervical radiculopathy, where an irritated or compressed nerve root causes arm pain, numbness, tingling, or weakness.
Lumbar Facet Joint Syndrome
When facet joints in the lower back are painful, patients often describe low back stiffness, pain with standing, pain with walking, discomfort when bending backward, or pain that may refer into the buttock or upper thigh.
Lumbar facet pain can overlap with back pain, spinal instability, spondylolisthesis, and degenerative disc disease.
Symptoms of Facet Joint Syndrome
The symptoms of facet joint syndrome vary by spinal region. The pain is often movement-related and may worsen with extension, rotation, or prolonged standing.
- Cervical facet pain: Neck stiffness, pain with turning the head, headaches, upper neck pain, trapezius pain, or shoulder blade discomfort.
- Thoracic facet pain: Mid-back pain, often worse with rotation, extension, or prolonged posture.
- Lumbar facet pain: Low back pain, stiffness, pain with standing or bending backward, and referred pain into the buttocks or upper thighs.
Facet pain may also trigger protective muscle spasms. Patients may feel tightness in the neck, upper back, or low back because the muscles are guarding an irritated joint.
Facet Joint Pain vs Pinched Nerve Pain
This is one of the most important distinctions for patients to understand.
Facet joint pain usually causes local or referred pain. It may spread into nearby areas, such as the shoulder blade, buttock, or upper thigh, but it usually does not follow a clear nerve-root pattern.
Pinched nerve pain, also called radiculopathy, often travels farther. In the neck, this may cause arm pain, numbness, tingling, or weakness. In the low back, it may cause sciatica-like pain traveling below the knee into the leg or foot.
If your symptoms travel from the neck into the arm or hand, review our page on cervical radiculopathy. If your symptoms travel from the low back into the leg, see our page on sciatica.
How Facet Joint Syndrome Is Diagnosed
Diagnosis begins with a detailed history and physical examination. We look at where the pain is located, what movements worsen it, whether pain travels into the arm or leg, and whether there are neurological symptoms such as numbness, weakness, or reflex changes.
Clinical Clues That Suggest Facet Joint Pain
- Pain that worsens with extension or rotation
- Localized tenderness near the spine
- Morning stiffness or pain after inactivity
- Pain that does not follow a classic nerve-root pattern
- Negative or limited nerve tension signs when radiculopathy is not present
- Referred pain to the shoulder blade, buttock, or upper thigh rather than true dermatomal pain
These clues can raise suspicion for facet-mediated pain, but they are not definitive. Many spine conditions overlap. Imaging and diagnostic injections are often needed to clarify the pain source.
Why MRI Alone Is Not Enough
MRI and CT scans can show arthritis, bone spurs, joint enlargement, inflammation, or degeneration. However, imaging findings do not always prove that the facet joint is the true source of pain.
Many patients have degenerative changes on imaging without significant pain. Others have pain from structures that look only mildly abnormal. For this reason, the diagnosis of facet-mediated pain usually requires matching the imaging with the symptom pattern, physical exam, and response to diagnostic blocks.
Medial Branch Blocks: The Key Diagnostic Test
The facet joints are supplied by small nerves called medial branch nerves. A medial branch block places a small amount of local anesthetic near these nerves under image guidance.
If the patient experiences meaningful temporary pain relief during the expected anesthetic window, the facet joint becomes a more likely source of pain.
In many cases, diagnostic medial branch blocks are performed in a stepwise fashion before proceeding to radiofrequency ablation. Some protocols use confirmatory blocks to improve diagnostic accuracy and reduce the chance of treating the wrong pain generator.
Why Are Medial Branch Blocks Sometimes Repeated?
Facet pain diagnosis can be challenging because back and neck pain are influenced by many factors. A single injection may occasionally produce temporary improvement because of placebo response, spread of anesthetic to nearby tissues, or natural symptom fluctuation.
Repeating the diagnostic block can help confirm that pain relief is consistent and reproducible. This is especially important before radiofrequency ablation, because RFA is most appropriate when the facet joint has been carefully confirmed as the pain source.
Treatment Options for Facet Joint Syndrome
Conservative Care
Many patients begin with non-surgical care. This may include:
- Physical therapy focused on mobility, posture, and stabilization
- Anti-inflammatory medications when medically appropriate
- Activity modification
- Weight management when relevant
- Heat, ice, and home exercise programs
- Ergonomic changes for desk work or driving
For cervical facet pain, therapy may focus on deep neck flexor strength, scapular mechanics, and posture. For lumbar facet pain, therapy often focuses on core stabilization, hip mobility, and reducing painful extension loading.
Facet Joint Injections
A facet joint injection places medication directly into or near the painful joint. This may be used in selected cases to reduce inflammation and pain.
Facet joint injections can sometimes help patients participate more effectively in physical therapy. However, when the goal is to confirm whether the joint is truly the pain source, medial branch blocks are often preferred.
Medial Branch Blocks
Medial branch blocks are primarily diagnostic. They can also provide short-term relief. A strong temporary response helps identify patients who may be candidates for radiofrequency ablation.
Radiofrequency Ablation
Radiofrequency ablation, also called RFA, uses controlled heat to reduce pain signals from the medial branch nerves that supply painful facet joints.
RFA does not remove arthritis or reverse degeneration. Instead, it quiets the pain pathway from a confirmed facet pain generator. In well-selected patients, relief may last months or longer. The nerve can regenerate over time, so the procedure may be repeated if pain returns and the patient continues to meet appropriate criteria.
Regenerative Options
Some patients ask about regenerative options such as platelet-rich plasma or other biologic therapies. These may be considered selectively, especially when inflammation, ligament irritation, or joint-related degeneration is suspected.
Evidence for regenerative treatments in spinal facet pain is still developing. These options should be discussed carefully, including expected benefits, limitations, cost, regulatory status, and whether the treatment is appropriate for the patient’s specific diagnosis.
Advanced Minimally Invasive Options
Some advanced procedures may be considered for carefully selected patients with recurrent facet-mediated pain, structural facet overgrowth, or limited benefit from standard care. These may include endoscopic or minimally invasive approaches aimed at treating painful facet-related anatomy.
Because these approaches are more specialized, they should be discussed on a case-by-case basis after diagnostic confirmation and review of imaging.
Spinal Fusion
Spinal fusion is generally not the first-line treatment for isolated facet joint syndrome. Fusion may be considered when facet pain occurs together with significant structural instability, deformity, spondylolisthesis, severe stenosis, or other surgical indications.
For isolated facet-mediated pain, less invasive treatments such as physical therapy, diagnostic blocks, and radiofrequency ablation are typically considered before major surgery.
Facet Pain Patterns: Choose What Fits Best
Prognosis and Long-Term Outlook
The outlook for facet joint syndrome is often favorable when the diagnosis is accurate and treatment is targeted. Many patients improve with a combination of posture correction, strengthening, activity modification, and image-guided interventions.
For patients who respond well to diagnostic medial branch blocks, radiofrequency ablation can provide a non-surgical option for longer-term pain relief. Because facet-related pain may recur over time, long-term management often includes exercise, ergonomics, weight control, and periodic reassessment.
Dr. Amit Sharma and the SpinePain Solutions team evaluate facet joint syndrome, cervical facet pain, lumbar facet pain, and related spine conditions across Long Island.
Schedule a consultation
Dr. Amit Sharma & our minimally invasive pain & spine team.
Frequently Asked Questions About Facet Joint Syndrome
What does facet joint pain feel like?
Facet joint pain often feels like aching, stiffness, or localized spine pain. In the neck, it may cause headaches or shoulder blade discomfort. In the lower back, it may refer into the buttock or upper thigh.
Can facet joint syndrome cause arm or leg pain?
Facet pain can refer into nearby areas, but it usually does not follow a classic nerve-root pattern. Arm pain with numbness, tingling, or weakness may suggest cervical radiculopathy. Leg pain traveling below the knee may suggest sciatica or lumbar radiculopathy.
How is facet joint syndrome diagnosed?
Diagnosis is based on symptom pattern, physical examination, imaging, and response to diagnostic medial branch blocks. MRI can show arthritis, but imaging alone does not prove the facet joint is the pain source.
Why are medial branch blocks done before radiofrequency ablation?
Medial branch blocks help confirm whether the facet joints are the likely pain source. If numbing the medial branch nerves provides meaningful temporary relief, radiofrequency ablation may be considered.
How long does radiofrequency ablation last for facet pain?
Relief varies by patient. In well-selected patients, RFA may provide relief for several months or longer. The treated nerves can regenerate over time, so symptoms may return.
Is facet joint syndrome the same as spondylosis?
Not exactly. Spondylosis is a broad term for age-related spinal degeneration. Facet joint syndrome refers more specifically to pain arising from the facet joints.
Is surgery needed for facet joint syndrome?
Surgery is not usually the first-line treatment for isolated facet pain. Fusion may be considered only when there are other structural problems such as instability, deformity, severe stenosis, or spondylolisthesis.
References
- Hurley RW, et al. Consensus practice guidelines on interventions for cervical spine facet joint pain. Regional Anesthesia & Pain Medicine. 2021.
- Cohen SP, et al. Consensus practice guidelines on interventions for lumbar facet joint pain. Regional Anesthesia & Pain Medicine. 2020.
- Perolat R, et al. Facet joint syndrome: from diagnosis to interventional management. Insights into Imaging. 2018.
- CMS Local Coverage Determination: Facet Joint Interventions for Pain Management.
- Wu J, et al. Platelet-rich plasma for lumbar facet joint syndrome: randomized controlled trial. Pain Practice. 2018.



