
Nimbus RFA Radiofrequency Ablation
Nimbus RFA: 5 Powerful Reasons It’s Changing Spine Care
Nimbus RFA: The Nimbus RFA cannula is a specialized radiofrequency ablation tool designed to treat chronic pain caused by facet joint arthritis and nerve irritation. Unlike traditional RFA probes, the Nimbus RFA cannula delivers a wider, more spherical lesion using a combination of monopolar and bipolar energy. This allows for more complete nerve targeting with fewer probe repositionings, which may result in longer-lasting relief for patients. At SpinePain Solutions, we use the Nimbus RFA system for neck, mid-back, and low back pain when conservative treatments fail.
Introduction
Neuro-destructive procedures have been used to treat medical conditions for over a century. Nerves carry pain signals, and targeted destruction of nerve tissue can achieve reduction or elimination of pain signals reaching the brain. Historically, alcohol or phenol was used as agents to destroy nerve cells. Injection of these agents is uncontrolled and unpredictable, even when small volumes are used. Radiofrequency neurotomy or ablation (RFN or RFA) was invented to destroy nerve tissue in a more controlled manner. Radiofrequency currents generate heat. These currents, when delivered through a needle, can create precise thermal lesions leading to tissue destruction. Skillfully created targeted lesions can selectively destroy nerves responsible for transmitting and/or modulating the signals of pain.
RFA is an established treatment which continues to evolve since its invention in the early 1970s. The treatment was initially used to treat back and neck pain originating from facet joints. Over the last decade, its use has expanded to treat several other pain syndromes, including chronic joint pain conditions affecting sacroiliac joints, shoulders, hips, and knees. I will spend a few minutes explaining the differences in various RF options.
Types of Radiofrequency Ablation
Conventional Continuous Radiofrequency (CRF)
CRF uses high-frequency alternating current to induce coagulative necrosis in the target tissue. Tissue destruction occurs at probe temperatures between 60° and 80° C. With CRF, the magnitude of tissue destruction is related to the temperature of the tissue, the size of the electrode as well as the duration of the procedure.
Not in the distant past, we were making lesions using a thin 22-gauge insulated needle with an active tip to create lesions near sites where medial branches are “supposed to” run. The procedure is done under fluoroscopic guidance. X-ray guidance can only help to guide positioning of the needle tip at the desired location. We cannot see these nerve branches. Depending on doctors’ preference, 1-3 lesions are created at each site to “capture” as many nerve branches as feasible. Higher numbers of lesions lead to better and longer lasting results.
Pulsed Radiofrequency (PRF)
PRF was introduced in 1998. PRF uses streams of radiofrequency current in short high-voltage bursts (20 ms) followed by the “silent” phase (480 ms) which allows time for heat elimination, generally keeping the target tissue below 42°C. Histopathologic work has shown that PRF at 42°C causes only transient endoneurial edema, while destructive wallerian degeneration is seen with CRF at 80°C. Since thermal damage from PRF is minimal and not how PRF exerts its clinical effect, it can be used at mixed sensory and motor nerves (like sciatic nerve), and even dorsal root ganglion. We are successfully using this technique to treat chronic radicular pain, ilioinguinal, genitofemoral and intercostal neuralgia.
Large Volume Radiofrequency (LVRF)
As the understanding of better results with larger lesions grew, there was a growing demand for needles that could create bigger legions. Coolief, Venom, Trident, SideKick and, more recently, Nimbus RFA needles have been introduced to achieve this goal. Of all these names, the Nimbus RFA needle creates the biggest lesion in the shortest amount of time. We recently introduced the Nimbus RFA cannula to Long Island for the very first-time.
Water-Cooled Radiofrequency (WCRF)
Water-Cooled radiofrequency ablation method (Coolief) also uses targeted heat lesions, but the needle tip is “cooled” to slightly lower temperatures (60°C, instead of 80°C) with constant flow of water. The slightly lower temperatures achieved with this system allowed for larger lesions to be performed without inducing tissue charring. Unfortunately, most clinicians report equipment problems complicating the treatment. The procedure takes longer, and equipment troubles are not uncommon during multi-lesion technique.
Nimbus RFA
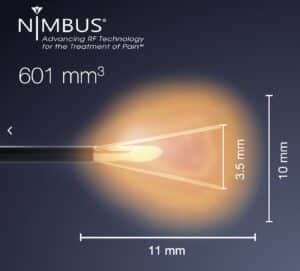
The Nimbus RFA needle was developed in 2009 by a Denver pain specialist, Dr. Robert Wright, who used his wife’s four-prong gem tweezers to create the first tined needle concept. The lesion created by his experimental device was consistently globular or cloud-shaped, hence the name, “Nimbus.” In contrast to Coolief, Nimbus RFA technique is far less cumbersome. The Nimbus RFA needle creates the largest volume of targeted lesion of all available options on the market. Our early results from using this needle and system have been nothing but spectacular. At present, we are the only group on Long Island using this device.
According to Stratus Medical, the manufacturer of the Nimbus RFA system, this cannula produces up to 8× the lesion volume compared to standard probes.
For further reading, refer to this NIH review on radiofrequency ablation discussing lesion creation methods and effectiveness.
 |
 |
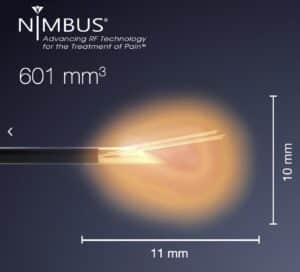 |
| Nimbus RFA Needle with deployable tines and the large lesion it creates. Courtesy: Stratus Medical |
||
Considering Nimbus RFA?
Dr. Amit Sharma and the team at SpinePain Solutions proudly introduced Nimbus RFA to Long Island. Discover if you’re a candidate for this next-generation treatment for chronic spine or joint pain.
Considering More Durable Relief? Medial Branch Neurectomy May Be the Answer
While Nimbus RFA is a powerful solution for many patients suffering from facet joint pain, some individuals may benefit from an advanced procedure known as Medial Branch Neurectomy. This minimally invasive technique not only targets the medial branch nerves responsible for pain but also addresses the underlying joint itself through a process called facet debulking.
At SpinePain Solutions, we frequently recommend Medial Branch Neurectomy for patients who:
- Have failed previous rounds of traditional or Nimbus RFA
- Experience recurrent or rapidly returning symptoms after nerve ablation
- Show significant facet joint hypertrophy on imaging studies
- Seek a longer-lasting alternative to repeated ablation procedures
Unlike RFA, which cauterizes the nerve, Medial Branch Neurectomy physically transects the medial branch nerve and removes excess joint overgrowth, helping reduce the likelihood of nerve regrowth and future joint irritation.
Studies have demonstrated that Medial Branch Neurectomy may provide pain relief lasting 12 to 24 months or longer, often exceeding the typical duration of relief achieved with RFA alone. This technique is especially well-suited for individuals seeking to minimize the need for repeat procedures and maximize the durability of their outcomes. Schedule a consultation to learn whether Medial Branch Neurectomy is a more appropriate solution for your spine care needs.
Conclusion
Radiofrequency ablation remains one of the bedrock foundational techniques of interventional pain medicine. We have been using this procedure to successfully treat neck, mid-back and lower back pain related to facet syndrome for decades. Refinements of this technique have extended its use to treat chronic pain syndromes related to joint pain (sacroiliac, shoulder, hip, knee) and many neuropathic pain conditions. We have proudly introduced the latest advancements of RFA on Long Island as a testament of our quest for perfection.



