Spondylolisthesis: 5 Critical Facts Every Patient Should Know
Spondylolisthesis occurs when one of the bones of the spine (a vertebra) slips out of its normal position relative to the bone below it. When the displaced vertebra shifts forward (anterolisthesis) or backward (retrolisthesis/posterolisthesis), it can narrow the spinal canal or foramen and may compress nearby spinal nerves, leading to back pain, leg pain, or neurologic symptoms. While spondylolisthesis can technically happen anywhere in the spine, it most commonly affects the lumbar (lower back) region, especially at the L4–L5 or L5–S1 levels.
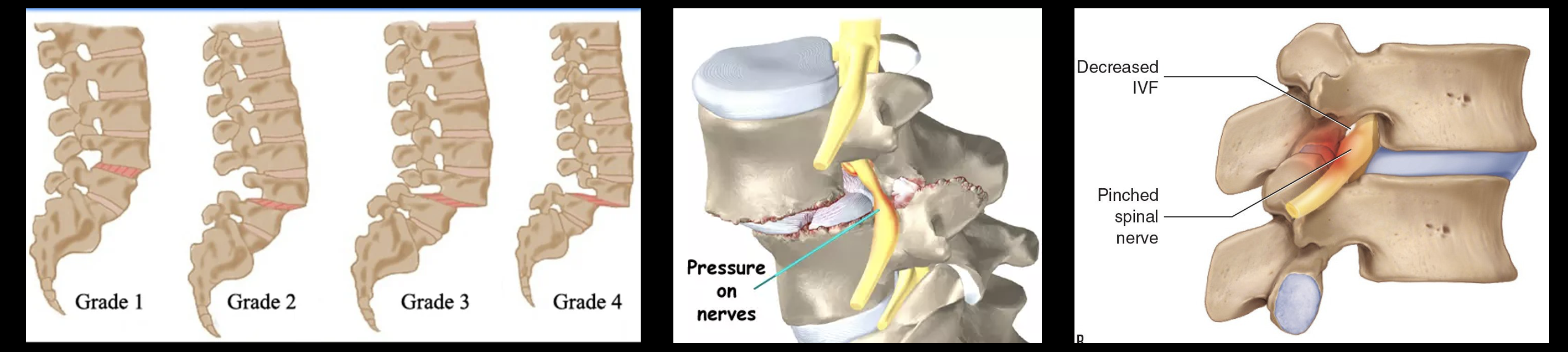
Radiologists often grade the amount of slippage using the Meyerding system: Grade I being the mildest displacement and Grade IV the most severe. Understanding the type and grade of spondylolisthesis helps guide decisions between conservative care, minimally invasive procedures, and surgery. For additional general background, organizations such as the American Academy of Orthopaedic Surgeons (AAOS) provide patient information about adult spondylolisthesis on their
OrthoInfo site.
1. What Is Spondylolisthesis?
The term “spondylolisthesis” comes from Greek—“spondylo” meaning spine and “listhesis” meaning slip. In simple terms, it refers to one vertebra slipping relative to the one below—most often forward (anterolisthesis), but sometimes backward (retrolisthesis/posterolisthesis). This loss of alignment can create instability and, in some patients, pressure on nerves.
Spondylolisthesis most commonly affects the lower lumbar vertebrae, particularly at the L4–L5 or L5–S1 levels. It can result from age-related degeneration, defects or stress fractures in the pars interarticularis (isthmic spondylolisthesis), congenital abnormalities, trauma, or underlying bone disease. Some patients never develop symptoms; others experience significant back and leg pain.
Types Of Spondylolisthesis
Doctors classify spondylolisthesis based on the underlying cause. The major types include:
-
Isthmic
Isthmic spondylolisthesis is usually related to a defect or stress fracture in a small area of bone called the pars interarticularis. This often begins as spondylolysis (a small crack in the pars), frequently in adolescence or young adulthood, especially in athletes who perform repetitive hyperextension (gymnasts, football linemen, weightlifters). Over time, the weakened segment may allow the vertebra to slip forward. Many patients remain asymptomatic for years and only develop symptoms later in life.
-
Degenerative
Degenerative spondylolisthesis is the most prevalent form in adults. It develops as discs lose height and the facet joints wear down with age. As the joints and ligaments become lax, a vertebra may gradually slip forward. This type is often associated with spinal stenosis and neurogenic claudication (heaviness or aching in the legs when walking).
-
Dysplastic
Dysplastic spondylolisthesis results from a rare congenital abnormality in which the lumbosacral joint is malformed from birth. This abnormal anatomy increases the risk of vertebral slippage, sometimes at a younger age.
-
Traumatic
Traumatic spondylolisthesis is usually caused by a high-energy injury that fractures or disrupts the supporting structures of the spine, allowing a vertebra to slip out of place. This variety is uncommon and often associated with other significant injuries.
-
Pathologic
Pathologic spondylolisthesis occurs when bone is weakened by an underlying condition such as osteoporosis, infection, or tumor. As the bone loses strength, it may no longer support normal spinal alignment, resulting in a slip.
Understanding Spondylolisthesis Nomenclature: A Simple “Diagnosis Recipe”
One reason spondylolisthesis terminology gets confusing is that clinicians often mix three different “labels” that describe different aspects of the same condition. The easiest way to keep it straight is to treat the diagnosis like a 3-part recipe:
1) Cause / Type (WHY): degenerative, isthmic, traumatic, dysplastic, pathologic, iatrogenic.
2) Direction (WHICH WAY): anterolisthesis (forward) vs retrolisthesis/posterolisthesis (backward).
3) Severity (HOW MUCH): commonly Meyerding Grade I–V (or percent translation).
Key point: Anterolisthesis/retrolisthesis are direction terms, not “types” of spondylolisthesis.
They can be paired with any cause. For example, someone can have degenerative spondylolisthesis with anterolisthesis, or degenerative spondylolisthesis with retrolisthesis. Meanwhile, isthmic slips are very commonly anterolisthesis because a pars defect tends to allow forward translation.
- Degenerative spondylolisthesis with Grade I anterolisthesis at L4–L5
- Degenerative spondylolisthesis with retrolisthesis at L3–L4
- Isthmic spondylolisthesis with Grade II anterolisthesis at L5–S1
If you only remember one thing, remember this: “Type” answers WHY, “-listhesis” direction answers WHICH WAY, and grade answers HOW MUCH.
Using all three makes imaging reports and treatment plans much easier to interpret.
2. What Are the Symptoms?
Many people with spondylolisthesis have no symptoms early on and are only diagnosed when imaging is obtained for another reason. When symptoms do occur or progress, they may include:
- Lower back pain that worsens with standing, extension, or activity
- Pain radiating into the buttocks or thighs
- Leg pain, numbness, tingling, or weakness (from nerve compression)
- Upper leg or calf fatigue with walking (neurogenic claudication)
- Tight hamstring muscles and difficulty bending forward
- Extreme tenderness at the slippage site
- Stiffness or a feeling of instability in the lower back
If untreated, significant spondylolisthesis can lead to postural changes such as exaggerated lordosis (swayback) or, in severe deformity, compensatory kyphosis (hunchback). In rare, advanced cases, severe nerve compression can cause problems with balance, walking, or even bladder and bowel function.
Red flag symptoms—such as progressive leg weakness, loss of bowel or bladder control, or saddle anesthesia—require urgent evaluation, as they may indicate severe nerve or cauda equina compression.
3. How Is Spondylolisthesis Diagnosed?
Diagnosis begins with a careful medical history and physical examination. Your spine specialist will ask about the onset and pattern of your pain, activities that worsen or relieve symptoms, prior injuries, and any neurologic symptoms such as leg weakness or numbness.
On examination, your physician may check:
- Posture and spinal alignment
- Range of motion and whether extension worsens symptoms
- Hamstring tightness and hip mobility
- Neurologic status (strength, sensation, and reflexes)
- Pain with raising a straightened leg, which may suggest nerve involvement
Spinal X-rays are crucial to detecting fractures, defects in the pars interarticularis, and misalignment of vertebrae. Standing and sometimes flexion/extension views can show how much the vertebra moves. Advanced imaging such as CT and MRI scans can reveal the degree of nerve involvement, spinal stenosis, and overall spinal architecture. In select cases, image-guided diagnostic injections are used to confirm the true source of pain.
4. What Treatments Are Available?
Treatment for spondylolisthesis depends on the type of slip, its severity, and the symptoms. Many patients improve with a combination of conservative and minimally invasive therapies before surgery is ever considered.
Conservative care may include:
- Physical therapy to strengthen the core and back muscles, improve flexibility, and reduce stress on the slipped segment.
- Medications such as anti-inflammatories, neuropathic agents, or short-term muscle relaxants to manage pain and inflammation.
- Activity modification, lumbar bracing, and posture education.
Minimally invasive and interventional options may include:
- Epidural steroid injections to reduce nerve-related leg pain (radiculopathy).
- Medial branch blocks and radiofrequency ablation when painful facet joints contribute to symptoms.
- Minimally invasive stabilization procedures such as the Minuteman® device in carefully selected patients.
- Endoscopic spine surgery to decompress nerves through very small incisions, with less disruption of supporting tissues.
Surgery is usually reserved for severe slippage, progressive neurologic deficits, or disabling pain that does not respond to comprehensive conservative care. Procedures may include decompression (removing bone or ligament compressing nerves) combined with fusion and instrumentation to stabilize the involved segment.
5. What Is the Outlook for Recovery?
With proper diagnosis and a tailored treatment plan, many patients with spondylolisthesis experience significant relief and return to daily activities. The outlook depends on the underlying cause, the degree of slippage, and how early treatment begins.
Patients with mild to moderate slips often do well with structured rehabilitation, targeted injections, and lifestyle changes. Minimally invasive interventions like selective nerve root blocks or facet joint blocks can provide both diagnostic information and symptom relief, and may delay or prevent the need for larger surgery in certain cases.
For patients who require surgery, advances in minimally invasive and image-guided techniques continue to improve recovery times and long-term outcomes. To learn more about treatment outcomes and rehabilitation from a national perspective, you may also review
Spine-Health’s treatment overview.
Summary
Spondylolisthesis is a broad but manageable spinal condition. Whether the slip is degenerative, isthmic, or related to another cause, early evaluation and a stepwise, minimally invasive treatment strategy can dramatically improve symptoms and function. Working with a spine specialist who understands both structural and nerve-related pain is the best way to avoid chronic disability and unnecessary surgery.
Dr. Amit Sharma and his minimally invasive pain & spine team provide advanced diagnostic testing and a full range of conservative, interventional, and surgical options to help you regain control and reduce pain.
Dr. Amit Sharma & our minimally invasive pain & spine team.



