
Basivertebral Nerve Ablation: 7 Breakthrough Benefits
Basivertebral nerve ablation is a minimally invasive treatment used for a specific type of chronic low back pain called vertebrogenic pain. In these patients, the pain may arise from the vertebral endplates and vertebral body rather than primarily from the disc, facet joints, or nerve roots.
When vertebral endplates become inflamed or damaged, the basivertebral nerve can transmit persistent pain signals from within the bone. This helps explain why some patients continue to have chronic low back pain despite treatments directed at other structures.
Basivertebral nerve ablation is designed to target that pain pathway directly. Rather than providing only temporary relief around the pain source, it treats the nerve associated with vertebrogenic pain. This treatment category includes established and newer platforms such as Intracept and OptaBlate.
What Is Basivertebral Nerve Ablation?
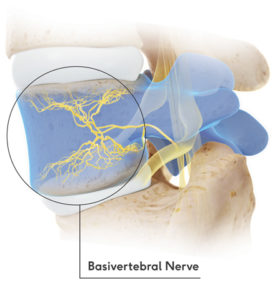 Basivertebral nerve ablation is a minimally invasive procedure designed to interrupt pain signals carried by the basivertebral nerve. This nerve lies inside the vertebral body and is closely associated with painful endplate changes seen on MRI, especially Modic type 1 and type 2 changes.
Basivertebral nerve ablation is a minimally invasive procedure designed to interrupt pain signals carried by the basivertebral nerve. This nerve lies inside the vertebral body and is closely associated with painful endplate changes seen on MRI, especially Modic type 1 and type 2 changes.
The procedure uses radiofrequency energy to create a controlled lesion around the basivertebral nerve, reducing its ability to continue transmitting pain signals. The goal is to address a specific source of vertebrogenic pain rather than temporarily calming nearby structures.
This treatment has gained attention because it provides both imaging correlation and a procedural strategy for a subset of chronic low back pain that was previously underrecognized.
Why Basivertebral Nerve Ablation Matters in Chronic Low Back Pain
Not all chronic low back pain comes from the same structure. Some pain is disc-related. Some is facet-mediated. Some is sacroiliac. Some is radicular and extends into the leg. Basivertebral nerve ablation matters because vertebrogenic pain is a distinct clinical category, and it requires a diagnosis-driven treatment approach.
Patients with vertebrogenic pain often report deep, midline axial low back pain, pain with sitting, pain with bending, and symptoms that have persisted despite conservative treatment. Many have already tried physical therapy, anti-inflammatory medication, activity modification, injections, or other procedures with only limited or temporary relief.
When the endplates and basivertebral nerve are the true pain generator, basivertebral nerve ablation may offer a more targeted option.
What Is Vertebrogenic Pain?
Vertebrogenic pain is pain arising from the vertebral endplates and vertebral body. The endplates are the interfaces between the discs and the vertebral bones. When these structures become inflamed, damaged, or degenerative, nociceptive signaling can increase, and the basivertebral nerve can transmit that pain.
This pattern is often associated with MRI findings called Modic changes. In general, Modic type 1 changes are associated with inflammatory change, while Modic type 2 changes are associated with fatty degeneration. These findings should always be interpreted in the context of the patient’s symptoms and clinical examination.
Vertebrogenic pain is different from classic sciatica. It is usually more axial and centered in the low back rather than primarily causing leg-dominant pain from nerve root compression.
Who Is a Candidate for Basivertebral Nerve Ablation?
A good candidate usually has chronic low back pain lasting at least six months, failure of conservative treatment, and MRI findings that support vertebrogenic pain. In many cases, the pain is predominantly axial, located in the lower lumbar region, and worsened by sitting, forward flexion, lifting, or sustained activity.
Patients often describe the pain as deep, aching, and mechanical. They may feel that it is different from muscle spasm and different from classic sciatica. Many have undergone multiple evaluations before the symptom pattern and MRI findings are finally recognized together.
Careful evaluation is essential. This treatment works best when the diagnosis is accurate.
Common features that may support candidacy
- Chronic low back pain persisting for 6 months or longer
- Failure of physical therapy, medication, or other conservative care
- Predominantly axial low back pain rather than primarily leg pain
- MRI showing Modic type 1 or type 2 changes
- Symptoms and imaging that fit a vertebrogenic pattern
How Basivertebral Nerve Ablation Is Performed
Basivertebral nerve ablation is performed using image guidance in a procedural setting. The vertebral body is accessed in a controlled fashion, and specialized instruments are used to reach the target region of the basivertebral nerve. Radiofrequency energy is then delivered to create a lesion that disrupts pain signaling.
The exact workflow depends on the platform being used. In general, the treatment is outpatient or same-day in nature. Most patients do not require a large incision. The procedure is designed to be precise, minimally invasive, and focused on the nerve pathway involved in vertebrogenic pain.
Recovery is usually measured in days for procedural soreness and weeks to months for the full benefit curve. Some patients notice change earlier, while others improve more gradually over time.
Basivertebral Nerve Ablation vs Traditional Treatments
Basivertebral nerve ablation differs from more familiar low back pain procedures because it targets a different pain source. Epidural injections are useful when inflamed nerve roots are driving symptoms. Facet blocks and medial branch radiofrequency ablation help when the facet joints are the source. Trigger point injections address myofascial pain. None of those treatments directly target the basivertebral nerve inside the vertebral body.
This does not make older treatments ineffective. It makes diagnosis essential. If the pain source is vertebrogenic, repeatedly treating discs, joints, or muscles may produce only limited or temporary benefit.
Basivertebral Nerve Ablation and Modic Changes
Basivertebral nerve ablation is especially relevant when MRI shows Modic changes that correlate with the patient’s symptoms. Modic changes are vertebral endplate and marrow signal changes seen on MRI, and they are an important part of the vertebrogenic pain discussion.
These findings do not automatically mean that every patient needs treatment, but when the history, examination, and MRI all align, they can be highly informative and can help guide a more targeted treatment strategy.
For some patients, careful review of the endplates changes the entire treatment conversation.
Intracept and OptaBlate: Two Approaches Within Basivertebral Nerve Ablation
Basivertebral nerve ablation is the treatment category. Intracept and OptaBlate are both platforms used to perform this procedure, and both are designed to target the same pain generator: the basivertebral nerve.
Intracept is the more established platform and is often the name patients encounter first when researching vertebrogenic pain. It has played an important role in bringing this diagnosis and treatment approach into broader clinical use.
OptaBlate is a newer platform within the same treatment category. While the technology and workflow may differ, the goal is the same: to treat vertebrogenic pain by addressing the basivertebral nerve within the vertebral body.
This is not a comparison of different conditions. It is a comparison of different ways to perform the same type of procedure. The most important factor is whether the diagnosis of vertebrogenic pain is correct.
Intracept
Intracept is a well-established basivertebral nerve ablation platform that many patients and referring physicians already recognize. It remains an important option within this treatment category.
OptaBlate
OptaBlate is another platform used to perform basivertebral nerve ablation. It provides an additional option for targeting the same underlying pain pathway in patients with vertebrogenic pain.
Benefits of Basivertebral Nerve Ablation
The main benefit of basivertebral nerve ablation is diagnostic alignment. It treats a recognized pain generator rather than repeatedly addressing nearby structures that may not be the true source of pain.
Potential benefits may include reduced pain, improved daily function, better sitting tolerance, improved ability to work or travel, and less dependence on repeated short-term interventions.
Many patients also find it helpful to finally understand the specific source of their pain and how it is being treated.
Recovery After Basivertebral Nerve Ablation
Most patients go home the same day after basivertebral nerve ablation. Mild soreness may occur from the procedure itself, but the larger question is how the underlying vertebrogenic pain changes over time. Relief may not be immediate and often builds over several weeks and sometimes longer.
Patients should follow specific post-procedure instructions from their treating physician. Activity progression, lifting limits, medication guidance, and return-to-work planning may vary depending on the individual case and the number of levels treated.
Setting expectations clearly is an important part of good care.
When Basivertebral Nerve Ablation Is Not the Right Fit
Basivertebral nerve ablation is not the correct treatment for every low back pain condition. If pain is primarily due to significant instability, fracture, infection, tumor, severe deformity, dominant radiculopathy, or another major structural issue, a different treatment plan may be more appropriate.
Likewise, if the MRI findings and symptom pattern do not support vertebrogenic pain, a different diagnosis should remain the focus.
The goal is not to fit every patient into one procedure. The goal is to determine whether basivertebral nerve ablation matches the actual pathology.
Basivertebral Nerve Ablation and Your Next Step
If you have chronic low back pain, MRI evidence of endplate change, and repeated short-lived relief from other treatments, basivertebral nerve ablation may be worth evaluating. The next step is a focused assessment that matches the history, examination, imaging, and prior treatment response to the actual pain generator.
You can learn more about vertebrogenic pain here and review the Intracept procedure page.
For additional outside reading, patients can review reputable information from Cleveland Clinic, the Stryker OptaBlate page, and peer-reviewed resources indexed through PubMed.



