Lumbosacral Transitional Vertebra: 7 Powerful Insights
Lumbosacral transitional vertebra (LSTV) is one of the most common – and most misunderstood – spinal findings on imaging. It is a congenital variant in which the lowest lumbar vertebra (usually L5) partially or completely “blends” with the sacrum, or the upper sacral segment behaves more like a lumbar vertebra. Many people have an LSTV and never develop pain.
Bertolotti Syndrome is different. It refers to back pain and/or leg pain that is clearly coming from a symptomatic LSTV – usually from a painful “pseudo-joint” between an enlarged transverse process and the sacrum or pelvis. In other words:
This landmark guide explains how to distinguish the two, why many patients are misdiagnosed, how true Bertolotti Syndrome is confirmed with targeted injections, and which minimally invasive treatments can help. For additional background on spinal anatomy and low back pain in general, large centers such as the Mayo Clinic and the American Academy of Orthopaedic Surgeons (AAOS) offer helpful overviews. This page focuses specifically on LSTV and Bertolotti Syndrome.
1. What Is a Lumbosacral Transitional Vertebra (LSTV)?
The lumbosacral junction is where the mobile lumbar spine meets the more rigid sacrum. In some people, this transition is altered by a congenital variant called a Lumbosacral Transitional Vertebra (LSTV). In simple terms, the lowest lumbar vertebra looks or behaves a little more like the sacrum – or the upper sacral segment behaves more like a lumbar vertebra.
There are two main patterns:
- Sacralization of L5 – L5 appears partially “fused” to the sacrum. The transverse processes (the side wings of the vertebra) are enlarged and may touch or join the sacrum or pelvis.
- Lumbarization of S1 – The first sacral segment looks more like an extra lumbar vertebra, increasing motion at the junction.
LSTV is common, occurring in an estimated 10–30% of the general population on imaging. Most people with an LSTV will never know they have it, and many never develop any symptoms. Problems arise when the abnormal connection between bone and sacrum behaves like a painful, overloaded joint.
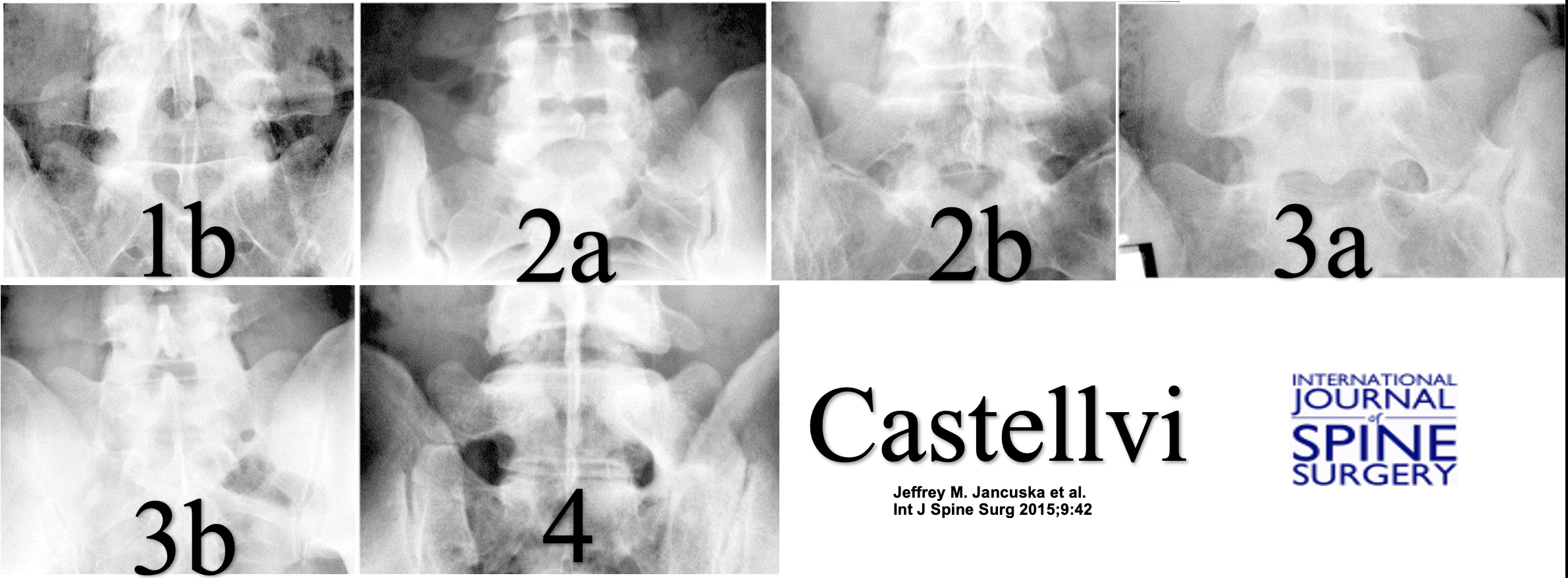
2. The Castellvi Classification: Why It Matters
Not all transitional vertebrae are the same. The Castellvi classification is the most widely used system to describe LSTV and is critical for proper diagnosis:
|
 |
For true Bertolotti Syndrome, the most clinically important categories are Type II and Type IV, where a pseudo-joint forms between the enlarged transverse process and the sacrum or pelvis and can become arthritic and painful over time.
3. LSTV vs. Bertolotti Syndrome: They Are Not the Same
One of the most important clarifications is this:
Having an LSTV on imaging does not automatically mean you have Bertolotti Syndrome.
LSTV describes a structural variant. It is a description of what your anatomy looks like on X-ray, CT, or MRI.
Bertolotti Syndrome is present only when:
- You have an LSTV and
- Your pain pattern and exam findings match involvement of that transitional segment and
- A targeted diagnostic injection into the pseudoarticulation (or related structures) significantly improves your pain.
In other words, Bertolotti Syndrome is a symptomatic subset of LSTV, not a synonym. Many people with LSTV have zero pain from it, and their back pain arises from more common sources like disc degeneration, facet arthritis, sacroiliac joint dysfunction, or muscular strain.
4. How Can a Lumbosacral Transitional Vertebra Cause Pain?
When an LSTV does become symptomatic, several mechanisms can be involved:
- Painful pseudoarticulation – In Castellvi Type II and IV variants, the enlarged transverse process forms a false joint with the sacrum or ilium. Over time, this pseudo-joint can develop arthritis, inflammation, and micro-motion that generates pain.
- Nerve irritation or compression – Hypertrophic bone or altered alignment can narrow the foramina or irritate nearby nerve roots, contributing to buttock or leg symptoms.
- Increased stress on the level above – Because motion is restricted at the transitional segment, the next level up (often L4–L5) may experience extra motion, leading to earlier disc degeneration, facet arthropathy, or spinal stenosis.
- Muscular and ligamentous overload – The iliolumbar ligament, quadratus lumborum, paraspinal muscles, and sacroiliac joint may become overloaded or imbalanced, further contributing to pain.
The key point is that an LSTV changes the normal biomechanics of the lower spine. In some people, this remains well tolerated. In others, especially those with a unilateral pseudoarticulation, the abnormal joint becomes a clear pain generator.
5. How Is True Bertolotti Syndrome Diagnosed?
A careful diagnosis goes far beyond simply seeing a large transverse process on an X-ray or MRI. A true diagnosis of Bertolotti Syndrome generally includes:
1. Accurate Anatomical Identification
- Confirming the presence and type of LSTV using X-ray (often with specialized Ferguson views) or CT.
- Using proper vertebral numbering (sometimes requiring whole-spine imaging or counting ribs) to avoid confusion.
- Classifying the transitional vertebra using the Castellvi system, with attention to Type II and Type IV pseudoarticulations.
2. Correlation With Symptoms and Exam
- Localized pain over the pseudoarticulation or lumbosacral junction.
- Symptoms aggravated by extension, rotation, or specific loading maneuvers.
- Frequently unilateral pain if only one side is involved.
- Consideration of other sources of pain, including sacroiliac joint dysfunction, L4–L5 disc disease, and facet joint arthritis.
3. Diagnostic Injection (Critical Step)
Image-guided injection is often the “gold standard” in confirming Bertolotti Syndrome. Under fluoroscopic or CT guidance, a small amount of local anesthetic – sometimes combined with steroid – is injected directly into the pseudoarticulation or clearly involved transitional segment.
Bertolotti Syndrome is strongly supported when:
- The injection reliably reaches the pseudoarticulation or target structure.
- The patient experiences significant, often dramatic, short-term pain relief in their typical pain pattern.
- Other potential pain sources have been reasonably evaluated and treated or ruled out.
Without this step, there is a real risk of incorrectly blaming the LSTV for pain that may actually be coming from a disc, facet joint, sacroiliac joint, or muscular source.
6. Treatment Options for LSTV and Bertolotti Syndrome
Treatment is individualized and depends on whether the LSTV is truly symptomatic, the severity of pain, the patient’s goals, and what other spinal conditions are present. Many patients benefit from a stepwise, minimally invasive approach.
Conservative Care
- Targeted physical therapy to improve core strength, hip and pelvic mechanics, and reduce stress on the transitional segment.
- Activity modification to avoid repetitive extension or loading that aggravates pain.
- Medication management using non-opioid strategies whenever possible.
Image-Guided Injections
- Diagnostic and therapeutic injections into the pseudoarticulation.
- Sacroiliac joint injections when SI joint overload coexists.
- Facet joint or medial branch injections if neighboring joints are also painful.
- Trigger point or ligament injections when myofascial or enthesis-related pain is present.
Radiofrequency Ablation (RFA)
In select patients, radiofrequency ablation can be considered to disrupt pain signals coming from the pseudoarticulation or associated nerves. This can offer longer-lasting relief than a single injection, particularly when diagnostic blocks have clearly confirmed the pain source.
When Is Surgery Considered?
Surgery is usually reserved for carefully selected patients with:
- Well-documented Bertolotti Syndrome confirmed by diagnostic injections.
- Persistent, disabling pain despite comprehensive conservative and interventional care.
- Clear correlation between the pseudoarticulation and symptoms.
Surgical options may include:
- Resection of the pseudoarticulation (removing the enlarged portion of the transverse process that forms the painful joint).
- Fusion of the involved segment in cases where there is significant instability or advanced degeneration of the adjacent level.
Importantly, surgery tends to have the best results when:
- The correct level is identified.
- The pseudoarticulation has been proven to be the main pain generator.
- Other major pain sources are not ignored.
7. Key Takeaways: Not Every LSTV Is Bertolotti Syndrome
To summarize:
- LSTV is a common anatomical variant at the lumbosacral junction, often discovered incidentally on imaging.
- Bertolotti Syndrome occurs only when an LSTV – typically a pseudoarticulation (Castellvi Type II or IV) – is clearly proven to be the source of pain.
- Not every enlarged transverse process or transitional segment is painful, and many people with LSTV never have symptoms.
- Accurate diagnosis requires a combination of imaging, careful examination, and targeted diagnostic injections.
- Treatment should be stepwise – beginning with conservative care and progressing to injections, radiofrequency ablation, or surgery only when truly indicated.
Working with a spine specialist who understands transitional anatomy, numbering pitfalls, and targeted diagnostic techniques is crucial to avoid both over-diagnosis and missed diagnosis of Bertolotti Syndrome.
Dr. Amit Sharma & our minimally invasive pain & spine team.
If you have been told that you have a “transitional vertebra,” “extra vertebra,” or “Bertolotti Syndrome” – or if you recognize your symptoms in this discussion – consider scheduling a consultation. A detailed, minimally invasive evaluation can help clarify whether your LSTV is truly the pain source and guide you toward the most precise treatment options.



