Sciatica vs SI Joint Pain: 3 Essential Clarity Tips
If you have deep pain in the lower back, buttock, or hip that sometimes radiates down the leg, it is natural to wonder whether the problem is coming from a pinched nerve in the spine or from the sacroiliac (SI) joint. Sciatica vs SI Joint Pain is a common clinical puzzle—even for experienced clinicians—and getting the diagnosis right is crucial because the treatments are very different.
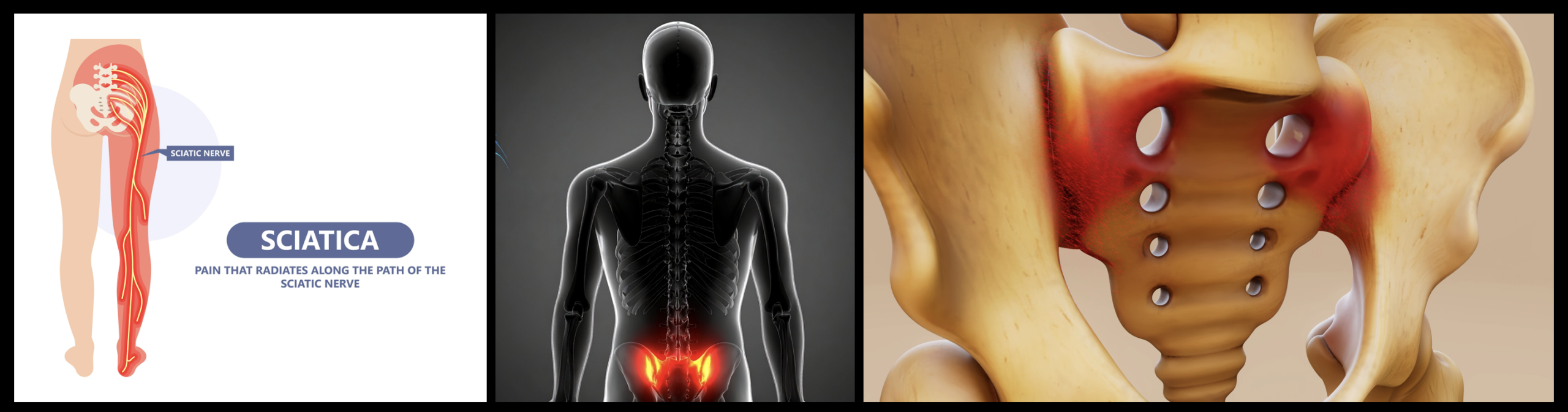
What Is Sciatica?
To understand Sciatica vs SI Joint Pain, it helps to define each condition clearly. Sciatica is a descriptive term for pain caused by irritation or compression of one or more nerve roots that form the sciatic nerve as they exit the lower spine. This is also called lumbar radiculopathy. When a disc herniation, bone spur, or spinal stenosis presses on these nerve roots, the irritated nerve can send shooting pain, tingling, numbness, or weakness down the leg.
Common causes of sciatica include:
- Lumbar disc herniation pressing on the L4, L5, or S1 nerve roots.
- Spinal stenosis (narrowing of the spinal canal or foramina).
- Degenerative disc and joint changes with bone spurs around the joints of the spine.
- Less commonly, tumors, cysts, infections, or fractures near the nerve root.
Typical features of sciatica include:
- Low back pain that may radiate into the buttock and leg.
- Shooting, electric, or burning pain that can travel below the knee and sometimes into the foot.
- Numbness, tingling, or “pins and needles” in a specific strip of skin (dermatome), such as the side of the calf or top of the foot.
- Possible weakness in certain muscle groups (e.g., difficulty lifting the foot or standing on tiptoes).
- Pain often worse with prolonged sitting, bending forward, lifting, coughing, or sneezing.
In the Sciatica vs SI Joint Pain comparison, sciatica generally points us toward a problem at the nerve root inside the spine rather than in the pelvic joints.
What Is SI Joint Pain?
The sacroiliac joints connect the base of the spine (sacrum) to the right and left iliac bones of the pelvis. SI joint pain occurs when these joints become inflamed, irritated, or move abnormally. This can be due to trauma, pregnancy-related ligament laxity, arthritis, prior lumbar fusion, or repetitive stress.
Common contributors to SI joint pain include:
- Falls or direct impact to the buttock or pelvis.
- Pregnancy and postpartum ligament laxity.
- Leg length differences or altered gait patterns.
- Inflammatory arthritis (such as spondyloarthropathies).
- History of lumbar fusion or other spine surgery that shifts load to the SI joints.
Typical features of SI joint pain include:
- Deep aching pain in the low back, just off to one side, or directly over the SI joint dimple area.
- Pain that may radiate into the buttock, hip, or upper thigh, but usually does not follow a strict nerve pattern to the foot.
- Worsening pain with prolonged standing, single-leg loading (standing on one leg), climbing stairs, or turning in bed.
- Relief when sitting or lying in certain positions, and aggravation with transitional movements (sit-to-stand, getting out of a car).
- Tenderness directly over the SI joint when pressed.
When thinking about Sciatica vs SI Joint Pain, SI joint pain behaves more like a mechanical joint problem at the base of the spine rather than a nerve root problem inside the spinal canal.
Essential Insights: Sciatica vs SI Joint Pain
Although both sciatica and SI joint pain can cause buttock and leg symptoms, several key insights help distinguish Sciatica vs SI Joint Pain during a careful evaluation.
Insight 1: Location and Pattern of Pain
- Sciatica: Pain often starts in the lower back or lumbosacral region and shoots down the buttock, back of the thigh, and past the knee. It may travel into the outer calf, top of the foot, or sole, depending on which nerve root is involved. The pattern usually follows a recognizable dermatome.
- SI Joint Pain: Pain is usually centered just off the midline at the posterior superior iliac spine (the “dimple” area) and can spread into the buttock, hip, and upper leg. It may cause a dull ache or sharp pain with certain movements but typically does not radiate in a clear, electric line all the way to the foot.
So in the Sciatica vs SI Joint Pain question, pain that reliably shoots below the knee and into the foot is more suggestive of sciatica, while pain focused around the SI region and buttock that rarely goes below the knee leans more toward SI joint involvement.
Insight 2: What Activities Make the Pain Worse
- Sciatica triggers: Bending forward, lifting, twisting, prolonged sitting (especially in a slumped position), and activities that increase disc and nerve root pressure often worsen sciatica.
- SI Joint Pain triggers: Standing or walking for long periods, going up and down stairs, standing on one leg, getting in or out of a car, or rolling in bed often aggravate SI joint pain. Many patients describe difficulty sitting with weight shifted onto one buttock.
Patients describing their own Sciatica vs SI Joint Pain often notice that sciatica crises flare with sitting and flexion activities, whereas SI joint pain is more provoked by weight-bearing and single-leg loading.
Insight 3: Physical Exam Clues and Provocative Tests
- Sciatica exam: Your specialist may find:
- Positive straight-leg raise or slump test that reproduces leg pain in a nerve pattern.
- Specific muscle weakness (e.g., foot drop, difficulty walking on heels or toes).
- Sensory changes in a defined dermatome.
- Altered reflexes at the knee or ankle.
- SI Joint exam: Findings often include:
- Localized tenderness directly over one or both SI joints.
- Pain reproduced by specific SI joint provocation tests (such as distraction, compression, thigh thrust, Gaenslen’s, or sacral thrust) when several are positive together.
- Normal strength and reflexes in the legs, aside from pain-limited effort.
In a structured Sciatica vs SI Joint Pain evaluation, the exam may show either clear radicular signs (favoring sciatica), clear SI provocation signs (favoring SI joint pain), or sometimes a combination that needs further testing.
Insight 4: Role of Imaging and Diagnostic Injections
- Sciatica imaging: Lumbar spine MRI can show disc herniations, stenosis, or other lesions compressing a nerve root. EMG/nerve conduction studies can further clarify whether symptoms match a specific radiculopathy.
- SI Joint imaging and injections: X-rays or CT may show SI joint degeneration or fusion, and MRI can show inflammation in some cases. However, imaging alone is often inconclusive. The most useful diagnostic tool for SI joint pain is often a fluoroscopically guided SI joint injection with local anesthetic—if pain relief is significant after numbing the joint, that strongly supports the SI joint as a major pain generator.
When Sciatica vs SI Joint Pain remains unclear after history, exam, and imaging, a combination of targeted nerve root injections or SI joint injections may help isolate which structure is actually responsible for your symptoms.
Insight 5: Can Both Sciatica and SI Joint Pain Coexist?
Yes. It is common for patients to have lumbar disc or facet disease plus SI joint overload from altered mechanics. In these combined Sciatica vs SI Joint Pain scenarios, one structure may have started the problem, and the other may have become painful secondarily.
Your provider may address the more dominant pain generator first, then reassess. For example, a patient might receive an epidural steroid injection for sciatica, followed later by an SI joint–focused rehab program or injection if a residual SI component remains.
Treatment Options: Sciatica vs SI Joint Pain
Once your evaluation clarifies where your pain is truly coming from, treatment can be tailored accordingly. Understanding Sciatica vs SI Joint Pain is therefore not just about naming the problem—it directly shapes your recovery plan.
Treatment for Sciatica
- Activity modification and self-care: Short periods of relative rest, then gradual return to activity; avoiding heavy lifting, twisting, and prolonged sitting.
- Medications: Anti-inflammatory medications, short courses of oral steroids when appropriate, neuropathic pain medications, and muscle relaxants.
- Physical therapy: Core strengthening, posture training, nerve mobilization techniques, and gradual conditioning focused on lumbar stability.
- Epidural steroid injections: Image-guided injections can decrease inflammation around an irritated nerve root and offer meaningful pain relief in carefully selected patients.
- Surgery: Reserved for progressive neurologic deficits, severe unremitting pain, or clear structural compression that has not responded to a comprehensive conservative plan.
If your symptoms and imaging clearly match the sciatica side of Sciatica vs SI Joint Pain, your plan may look similar to other targeted approaches used for back pain and sciatica, with the focus on calming the nerve root and stabilizing the spine.
Treatment for SI Joint Pain
- Physical therapy and exercise: Focused programs to strengthen the core, gluteal, and hip muscles; correct pelvic mechanics; and restore balanced loading across the SI joints.
- Activity modification: Avoiding prolonged single-leg loading, using proper lifting mechanics, and adjusting daily tasks that provoke SI stress.
- Supportive devices: In some cases, an SI belt or brace can help stabilize the pelvis during activity.
- Manual therapy: Hands-on techniques, mobilization, and myofascial work may help in selected patients when used alongside strengthening.
- Interventional procedures: Image-guided SI joint injections with local anesthetic and steroid can reduce inflammation and confirm the joint as a pain source. In patients who respond but have recurrent pain, radiofrequency ablation (RFA) of the lateral branches that supply the SI joint may provide longer-term relief in appropriately selected cases.
- Surgical options: Minimally invasive SI joint fusion is reserved for severe, persistent SI joint pain that has failed a thorough course of non-surgical care and appropriate injections.
When treatment is focused on the SI side of Sciatica vs SI Joint Pain, the emphasis is on stabilizing the joint, reducing inflammation, and restoring normal movement patterns across the pelvis and hips.
When to Worry and Seek Urgent Care
Regardless of whether your pain turns out to be on the sciatica or SI joint side of the Sciatica vs SI Joint Pain conversation, certain “red flag” symptoms should prompt urgent evaluation:
- Sudden, severe weakness in one or both legs.
- Loss of bowel or bladder control, or new numbness in the groin or saddle region.
- Fever, chills, unexplained weight loss, or history of cancer along with new back or leg pain.
- Back or pelvic pain after major trauma (such as a fall or car accident).
These symptoms are not typical of routine SI joint pain or uncomplicated sciatica and require immediate attention.
Next Steps: Clarifying Your Diagnosis and Building a Plan
Many people live for months thinking they have sciatica when the primary issue is actually the SI joint, and others focus on the pelvis when the real driver is a pinched nerve root. The goal of a thorough Sciatica vs SI Joint Pain evaluation is to match your unique story, physical exam, and imaging findings to the correct diagnosis so that each treatment—therapy, medication, injection, or procedure—is aimed at the true pain generator.
If you are unsure whether your symptoms fit better with sciatica or SI joint pain—or if you suspect a combination of both—consider a consultation with a fellowship-trained spine and pain specialist. A targeted approach can help you move from uncertainty and trial-and-error to a more precise, minimally invasive plan tailored to your goals and lifestyle.
Ready to Find the Real Source of Your Pain?
If you have ongoing low back, buttock, or leg pain and are not sure whether it is sciatica, SI joint pain, or a mix of both, a focused evaluation can make all the difference. By combining a detailed history, hands-on examination, and targeted imaging or injections when needed, we can clarify your personal Sciatica vs SI Joint Pain picture and design a plan around your specific needs.
Schedule a consultation to review your MRI, prior treatments, and daily activity demands so we can map out the safest and most effective next steps toward lasting relief.



