
Superior Cluneal Neuropathy
Understanding Superior Cluneal Neuropathy
Superior Cluneal Neuropathy is a frequently overlooked cause of chronic lower back pain. It results from irritation or entrapment of the superior cluneal nerves, which pass through the thoracolumbar fascia and innervate the skin over the posterior iliac crest and upper gluteal region.
This neuropathy can closely mimic conditions like lumbar disc herniation or sacroiliac joint dysfunction. Because it often goes unrecognized, patients may endure unnecessary imaging, procedures, or even surgery without relief. Understanding this condition is crucial to effective, minimally invasive treatment and pain resolution.
Symptoms of Superior Cluneal Neuropathy
Symptoms are often mistaken for lumbar radiculopathy or facet joint pain. Classic signs include:
- Sharp, burning, or aching pain over the iliac crest and upper buttock
- Increased pain with lumbar extension or prolonged standing
- Tenderness 7–8 cm lateral to midline over the iliac crest
- Relief with local nerve block injection
The pain does not typically radiate past the greater trochanter and is purely sensory, helping distinguish it from radiculopathy.
What Causes Superior Cluneal Neuropathy?
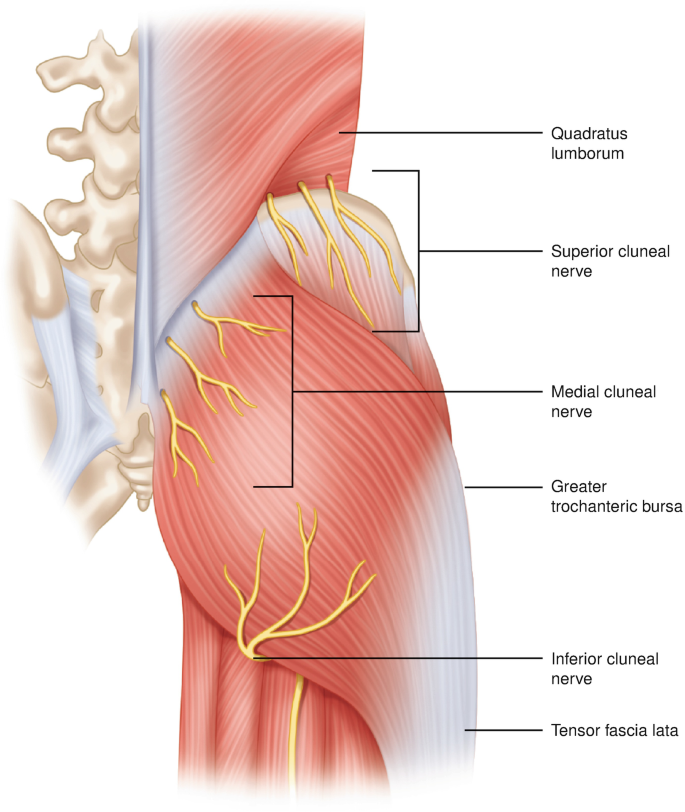 The superior cluneal nerves originate from the dorsal rami of the T11–L5 spinal nerves. These nerves pass through the rigid thoracolumbar fascia and are particularly vulnerable to entrapment at a fibrous tunnel 3–4 cm above the iliac crest.
The superior cluneal nerves originate from the dorsal rami of the T11–L5 spinal nerves. These nerves pass through the rigid thoracolumbar fascia and are particularly vulnerable to entrapment at a fibrous tunnel 3–4 cm above the iliac crest.
Common contributing factors include:
- Repetitive strain or mechanical trauma
- Thoracolumbar fascia thickening (e.g. from overuse or surgery)
- Scar tissue from prior lumbar procedures
- Prolonged standing or lumbar extension postures
How Is Superior Cluneal Neuropathy Diagnosed?
Diagnosis is primarily clinical and relies on detailed history and physical examination. Patients often describe focal tenderness over the posterior iliac crest. A key diagnostic maneuver is identifying a trigger point located approximately 7–8 cm lateral from the midline at the iliac crest.
Confirmatory diagnosis can be achieved by performing a diagnostic nerve block. If the patient experiences temporary pain relief after an injection with local anesthetic, it strongly supports the diagnosis of Superior Cluneal Neuropathy. PubMed: Ogura et al., 2008
Other conditions such as lumbar facet arthropathy, radiculopathy, and sacroiliitis should be ruled out using imaging or additional physical tests.
Effective Treatments for Superior Cluneal Neuropathy
Initial treatment for superior cluneal neuropathy is typically conservative and focuses on reducing mechanical irritation of the nerve. This includes activity modification, physical therapy directed at the lumbar spine and pelvis, and non-steroidal anti-inflammatory medications (NSAIDs). These approaches aim to improve biomechanics, reduce inflammation, and relieve pressure on the nerve.
However, because superior cluneal neuropathy is often caused by focal nerve irritation or entrapment, conservative measures alone may not fully resolve symptoms. When pain persists or when diagnostic clarity is needed, more targeted treatments are essential.
1. Superior Cluneal Nerve Block
A superior cluneal nerve block is one of the most important tools in both diagnosing and treating this condition. The procedure involves injecting a small amount of local anesthetic, often combined with a corticosteroid, around the superior cluneal nerves where they cross the iliac crest.
Why This Injection Matters
- Diagnostic confirmation: Significant improvement in the patient’s typical pain after the injection strongly supports the diagnosis of superior cluneal neuropathy.
- Differentiation: Helps distinguish cluneal nerve pain from sacroiliac joint dysfunction, lumbar radiculopathy, or piriformis syndrome.
- Real-time feedback: Provides immediate clinical insight when imaging findings are inconclusive.
Therapeutic Benefit
In addition to confirming the diagnosis, the injection may provide meaningful relief. Some patients experience substantial and sustained improvement after a single block, especially in early or less severe cases. In others, relief may be temporary but still extremely valuable in guiding further treatment.
When the response is positive but short-lived, repeat injections or additional nerve-targeted therapies may be considered.
For a detailed overview of the procedure and what to expect, see our dedicated page on cluneal nerve block.
Key clinical insight: Because these nerves are small and not easily visualized, a positive response to a nerve block is often one of the most reliable indicators that the superior cluneal nerves are the true source of pain.
2. Radiofrequency Ablation (RFA)
In patients with chronic symptoms who do not achieve lasting relief from conservative therapy or nerve blocks, radiofrequency ablation (RFA) may be considered. This procedure uses controlled thermal energy to disrupt pain signaling from the affected nerve branches.
- Minimally invasive: Performed using image guidance for precise targeting
- Longer-lasting relief: May provide months of symptom improvement in selected patients
- Best candidates: Patients who have demonstrated a positive response to diagnostic nerve blocks
Clinical studies, including findings reported by Matsumoto et al., suggest that RFA of the superior cluneal nerve can provide meaningful and sustained pain reduction in appropriately selected patients.
3. Regenerative Medicine Approaches
Emerging regenerative therapies aim to address the underlying tissue irritation and nerve inflammation rather than simply blocking pain signals.
- Platelet-Rich Plasma (PRP): Uses concentrated growth factors from the patient’s own blood to promote healing at the entrapment site
- Exosome-based therapies: Investigational approaches designed to modulate inflammation and support tissue repair
These treatments are considered off-label and are typically offered in specialized settings. They may be considered in carefully selected patients, particularly when conventional therapies have not provided sufficient relief.
While research is ongoing, regenerative approaches represent a promising direction in the management of nerve-related pain conditions such as superior cluneal neuropathy.
In practice, treatment is often individualized. Some patients respond well to conservative care alone, while others benefit from a combination of nerve blocks, interventional procedures, and targeted rehabilitation strategies.
Recovery Outlook
Patients receiving image-guided nerve blocks or radiofrequency ablation often report significant symptom relief within 1–2 weeks. Long-term outcomes are best when coupled with core strengthening, postural correction, and addressing thoracolumbar fascia mobility.
If conservative therapy fails and pain recurs, surgical decompression of the cluneal nerve entrapment site is rarely needed but may be considered in expert centers.
Chronic Back Pain? It Could Be Cluneal Neuropathy
Don’t let a missed diagnosis keep you in pain. At SpinePain Solutions, we specialize in diagnosing and treating Superior Cluneal Neuropathy with targeted, minimally invasive techniques.
Frequently Asked Questions
How common is Superior Cluneal Neuropathy?
It’s more common than previously thought and may account for 10–14% of chronic low back pain cases in specialized clinics.
Is imaging helpful in diagnosing Superior Cluneal Neuropathy?
Not typically. MRI or X-rays may help rule out other causes, but diagnosis is mostly clinical and confirmed with nerve blocks.
Can this condition return after treatment?
Recurrence can happen, especially if biomechanical issues are unaddressed. Long-term success improves with postural retraining and therapy.
References
- Henson, J., Merkow, J., Varhabhatla, N. (2022). Superior Cluneal Nerve Block. In: Souza, D., Kohan, L.R. (eds) Bedside Pain Management Interventions. Springer, Cham. https://doi.org/10.1007/978-3-031-11188-4_36.



