Isthmic Spondylolisthesis: 5 Powerful Insights for Patients
Isthmic spondylolisthesis occurs when a small region of bone in the back of the vertebra, called the pars interarticularis, develops a defect or stress fracture. Over time, this weakened area can allow one vertebra to translate—most often forward (anterolisthesis)—on the vertebra beneath it. This type of slippage most commonly affects the lower lumbar spine, especially at the L5–S1 level.
Isthmic spondylolisthesis often begins as spondylolysis—a crack or defect in the pars—usually during adolescence or early adulthood. It is especially common in athletes who perform repetitive lower-back extension, such as gymnasts, football linemen, dancers, divers, and weightlifters. While some individuals remain symptom-free for years, others may develop lower back pain, hamstring tightness, or leg symptoms as the slip progresses or as nerves become compressed.
For trusted national overviews of spondylolysis and spondylolisthesis, you may also review resources from the
American Academy of Orthopaedic Surgeons (AAOS) and the Mayo Clinic.
For a broader overview of ALL types of spondylolisthesis, you can also review our general Spondylolisthesis guide.
How to Describe Isthmic Spondylolisthesis Clearly (The “Diagnosis Recipe”)
A common terminology mistake is to treat anterolisthesis or retrolisthesis as if they are “types” of spondylolisthesis. They are not. They describe direction. “Isthmic” describes cause.
The cleanest way to keep this straight is to describe the diagnosis using three independent parts:
- Cause / Type (WHY): Isthmic = a pars interarticularis defect (spondylolysis) that allows translation.
- Direction (WHICH WAY): Anterolisthesis (forward) vs retrolisthesis/posterolisthesis (backward).
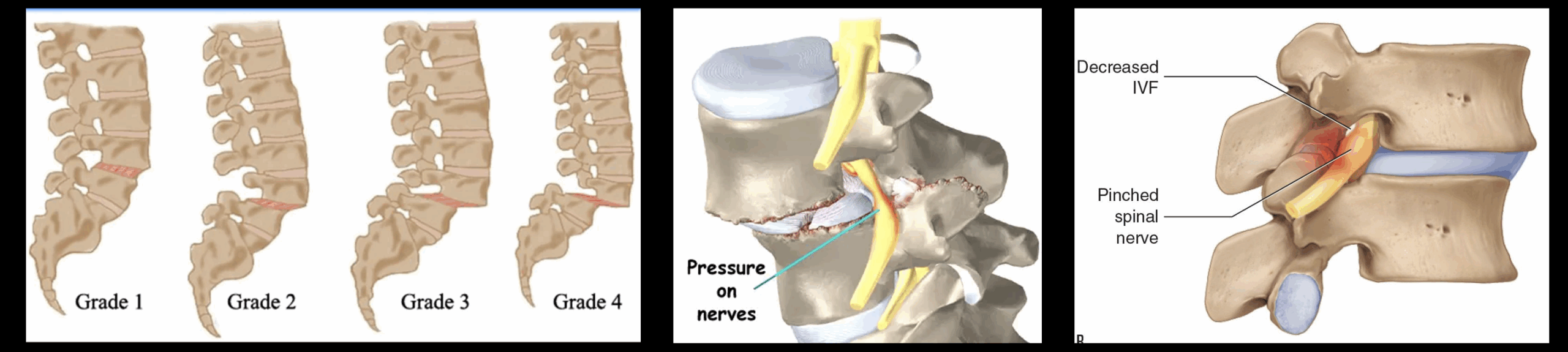
- Severity (HOW MUCH): commonly Meyerding Grade I–V (or percent translation).
Key point:
“Isthmic” is the type/cause. “Anterolisthesis/retrolisthesis” is the direction.
In real-world practice, isthmic slips are very commonly anterolisthesis because a pars defect tends to permit forward translation—especially at L5–S1.
How clinicians say it (complete examples):
- Isthmic spondylolisthesis with Grade I anterolisthesis at L5–S1
- Isthmic spondylolisthesis with Grade II anterolisthesis at L5–S1 with foraminal stenosis
1. What Is Isthmic Spondylolisthesis?
In isthmic spondylolisthesis, the underlying issue begins with weakening or failure of the pars interarticularis. Repetitive stress—especially from extension and rotation—can create or worsen a small fracture in this region. If the bone does not heal fully or remains unstable over time, the vertebra may slip forward, producing a measurable displacement.
Key characteristics of isthmic spondylolisthesis include:
- Most common at the L5–S1 level
- Frequently associated with repetitive athletic stress
- May develop in childhood but not cause symptoms until adulthood
- Slippage ranges from mild (Grade I) to more advanced (Grade II–IV)
- Direction is most often anterolisthesis, but direction and type are described separately
The forward slip can cause mechanical back pain and, in some cases, narrow the nerve openings (foramina), leading to irritation or compression of the exiting L5 nerve root.
2. Spondylolysis vs. Isthmic Spondylolisthesis
These two related terms describe different stages of the same underlying process:
- Spondylolysis — a defect or stress fracture in the pars interarticularis, usually without vertebral slippage.
- Isthmic spondylolisthesis — occurs when that weakened vertebra slips forward due to the pars defect.
Not all patients with spondylolysis progress to spondylolisthesis, but those who do may experience symptoms such as pain with extension, hamstring tightness, and neurologic symptoms when nerves become compressed.
Common risk factors include:
- High-impact or extension-based athletics
- Genetic predisposition or anatomic variation
- Repetitive loading without adequate rest or conditioning
3. Symptoms of Isthmic Spondylolisthesis
While some individuals remain asymptomatic, symptomatic isthmic spondylolisthesis may present with:
- Lower back pain that worsens with extension or prolonged standing
- Tight hamstrings and reduced flexibility
- Radiating buttock or leg pain due to nerve compression
- Numbness or tingling in the legs or feet
- Back muscle spasms or a feeling of instability
More advanced cases can interfere with athletic performance, daily activities, or gait. Rare but serious symptoms—such as progressive weakness, bowel or bladder changes, or saddle numbness—require urgent evaluation.
4. How Is Isthmic Spondylolisthesis Diagnosed?
Diagnosis begins with a thorough history and physical examination. Dr. Sharma evaluates spinal alignment, motion, hamstring flexibility, and neurologic function. Pain reproduced with lumbar extension is common in isthmic cases.
Imaging studies used to diagnose and evaluate the condition include:
- X-rays — Often show pars defects, slippage, or vertebral instability.
- Oblique X-rays — Can highlight the “Scotty dog” sign of a pars fracture.
- Flexion/extension films — Assess stability and motion at the slipped level.
- CT scans — Excellent for defining pars anatomy and fracture details.
- MRI scans — Reveal nerve compression, spinal stenosis, and disc health.
Image-guided injections—such as selective nerve root blocks or pars/facet region injections—may be used to pinpoint the exact pain generator and guide treatment.
5. Treatment Options for Isthmic Spondylolisthesis
Treatment is customized to the patient’s symptoms, slip severity, lifestyle, and goals. Many individuals—especially those with low-grade slips—do very well with conservative and minimally invasive approaches.
Conservative Care
- Physical therapy emphasizing core strength, hip mobility, and flexibility
- Medications for inflammation, muscle spasm, or nerve pain
- Activity modification or short-term bracing in select cases
Minimally Invasive & Interventional Options
- Epidural steroid injections for radiculopathy
- Selective nerve root blocks for diagnostic and therapeutic benefit
- Pars or facet injections for localized pain
- Minimally invasive stabilization procedures in carefully selected patients
When Is Surgery Necessary?
Surgery is considered when:
- There is a high-grade slip with deformity or instability
- Symptoms persist despite comprehensive conservative care
- Progressive neurologic deficits develop
Modern minimally invasive techniques allow for targeted decompression and stabilization with shorter recovery times and less tissue disruption.
6. Living With Isthmic Spondylolisthesis
Many patients continue to lead active, healthy lifestyles with appropriate care. Long-term success depends on core strengthening, flexibility, good biomechanics, and early attention to flare-ups.
With the right combination of rehabilitation, interventional treatments, and—when necessary—minimally invasive surgery, patients can achieve excellent long-term outcomes.
Dr. Amit Sharma & our minimally invasive pain & spine team.
If you have been told you have a pars defect, spondylolysis, or isthmic spondylolisthesis—or if your symptoms match those described—schedule a consultation today. Early diagnosis and precise treatment can prevent progression and dramatically improve quality of life.



