Radiculopathy: 7 Awesome Facts & Treatment Options
Radiculopathy is the medical term for symptoms that arise when a spinal nerve root is irritated or compressed as it exits the spine. This can feel like shooting pain, tingling, numbness, or weakness traveling from the neck or back into the arm or leg. Many patients know it simply as a “pinched nerve.”
On this page, you’ll learn what radiculopathy is, how it differs from sciatica, what symptoms to watch for, and the minimally invasive treatment options available with Dr. Amit Sharma on Long Island.
Page Overview
Who This Page Is For (and How to Use It)
- This page is for you if: You have arm or leg symptoms (pain, tingling, numbness, or weakness) and were told you may have a “pinched nerve,” disc issue, or sciatica.
- How to use this page: Start with the Quick Summary below, then jump to Radiculopathy vs Sciatica if you’re comparing diagnoses, or Treatment Options if you want to know next steps.
- Simple mental model: Think of spinal nerves like electrical cables leaving a wall. If the exit opening narrows or the nerve gets irritated, symptoms don’t always stay in the back or neck—they can travel down the “cable” into the arm or leg.
- Sudden or rapidly worsening weakness in an arm or leg
- Loss of control of bowel or bladder function
- Numbness in the groin or “saddle” region
- Severe, unrelenting pain with fever, chills, or unexplained weight loss
Radiculopathy Quick Summary
- What it is: Irritation or compression of a spinal nerve root, often called a “pinched nerve.”
- Common locations: Neck (cervical), mid-back (thoracic), and low back (lumbar).
- Typical symptoms: Radiating arm or leg pain, tingling, numbness, or weakness following a nerve pathway.
- Not just pain: Some people mainly notice numbness or weakness, with little or no back or neck pain.
- Treatment options: Activity modification, targeted physical therapy, medications, and image-guided procedures.
- Surgery: Reserved for selected cases with severe or progressive deficits or persistent symptoms.
What Is Radiculopathy?
Radiculopathy occurs when a spinal nerve root becomes inflamed, irritated, or compressed as it travels through a narrow bony tunnel (the foramen). Common causes include disc herniation, bone spurs from arthritis, thickened ligaments, spinal stenosis, or sometimes subtle instability in the spine. Not all narrowing on imaging causes symptoms, but when the nerve root is involved, patients may feel distinctive radiating patterns of pain, tingling, or weakness.
Different regions of the spine can be affected:
- Cervical: Nerve root irritation in the neck sending symptoms into the shoulder, arm, or hand.
- Thoracic: Less common; symptoms can wrap around the chest or upper abdomen.
- Lumbar: Often responsible for leg pain, including classic sciatica
7 Key Things to Know About Radiculopathy
1. It’s More Specific Than Just a “Pinched Nerve”
People often hear they have a “pinched nerve,” but radiculopathy refers specifically to dysfunction at the nerve root as it exits the spine. The nerve may be compressed by a disc herniation or bone spur, inflamed by chemical irritation from a damaged disc, or stretched by abnormal motion between vertebrae. Symptoms reflect that nerve’s job: sensation and muscle control in a particular pathway.
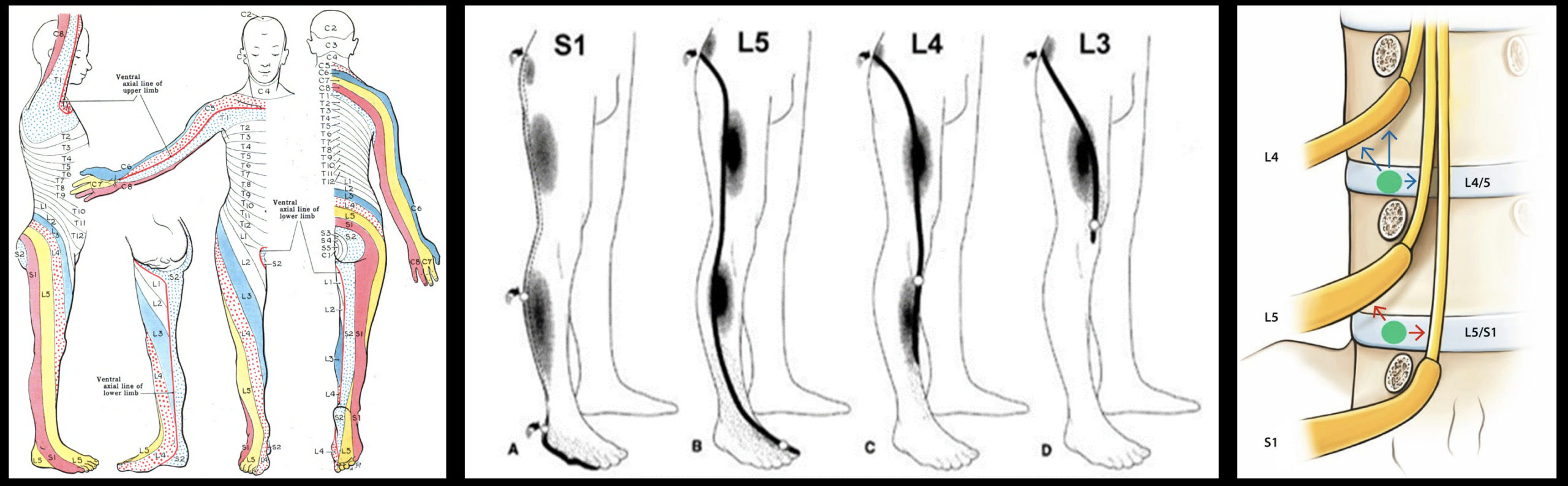
2. Symptoms Follow a Predictable Nerve Map
Nerve roots supply distinct “maps” of sensation and strength called dermatomes (areas of skin supplied by a specific nerve) and myotomes (muscle groups controlled by a specific nerve). When one root is affected, symptoms often follow a narrow track:
- Neck into shoulder and down the arm, possibly into specific fingers.
- Low back into the buttock, thigh, calf, or foot.
- Band-like pain around the chest or trunk for thoracic involvement.
This predictable pattern helps your physician identify which nerve root is likely involved before even looking at imaging.
3. Sciatica Is One Type of Radicular Leg Pain
Sciatica vs radiculopathy is a common question. The term “sciatica” usually refers to radiating leg pain from the lower lumbar nerve roots that contribute to the sciatic nerve. That makes it one specific form of lumbar nerve-root irritation. Radicular problems can also occur higher up in the lumbar spine or in the neck or mid-back, where there is no sciatic nerve at all.
In short:
- Radiculopathy: A nerve-root issue anywhere in the spine.
- Sciatica: Radiating leg pain from lower lumbar nerve roots that form the sciatic nerve.
4. It Is Not Always Primarily a Pain Condition
Some patients expect dramatic pain with nerve-root involvement, but others mainly notice sensory changes or weakness. Common complaints include:
- Persistent numbness or a “dead” feeling in part of the arm or leg.
- Tingling or pins-and-needles along a narrow strip of skin.
- Weakness gripping, lifting the arm, climbing stairs, or lifting the foot.
Even when pain improves, residual numbness or weakness can indicate ongoing nerve-root involvement and deserves careful monitoring.
5. Disc Findings on MRI Do Not Always Match Symptoms
Advanced imaging often shows disc bulges, herniations, or arthritic changes in people with no radiating symptoms. These are sometimes incidental. True nerve-root involvement typically requires:
- Symptoms that match a specific nerve map, and
- Exam findings and/or imaging that support that pattern.
This is why Dr. Sharma emphasizes correlating your story, physical exam, and imaging rather than treating the MRI alone. A dramatic-looking disc without matching symptoms may not be the true source of the problem.
6. Patterns Differ in the Neck, Mid-Back, and Low Back
Cervical nerve-root irritation may cause:
- Neck discomfort that may worsen with certain positions.
- Electric or burning sensations into the shoulder, arm, or hand.
- Numbness or tingling in specific fingers.
- Weakness lifting the arm, bending the elbow, or opening jars.
These symptoms overlap with cervicobrachial pain syndromes, in which muscles and joints can also contribute to the pattern.
Lumbar nerve-root problems often cause:
- Low back pain with shooting pain into the buttock or leg.
- A burning or electric sensation along the thigh, calf, or foot.
- Difficulty standing upright or walking for long distances.
- Weakness climbing stairs or lifting the foot.
Thoracic involvement is less common but may cause a band of pain wrapping around the chest or upper abdomen. Other conditions, such as hip arthritis or sacroiliac joint problems, can mimic these patterns and must be considered separately.
7. Many Patients Improve Without Major Spine Surgery
The encouraging news is that many people with nerve-root related symptoms improve over time with a combination of activity modification, targeted physical therapy, medications when appropriate, and image-guided procedures. Only a subset ultimately requires major surgery. Early, accurate diagnosis and a stepwise treatment plan help relieve symptoms and protect function while avoiding unnecessary interventions.
Common Symptoms by Region
Cervical Region (Neck and Arm)
- Neck discomfort with radiation into the shoulder, arm, or hand.
- Tingling or numbness in specific fingers.
- Weakness with reaching, lifting, or gripping objects.
- Occasional associated headaches or upper-back discomfort linked to neck mechanics.
Thoracic Region (Mid-Back and Chest)
- Band-like pain wrapping around the chest or upper abdomen.
- Burning or sharp pain between or around the ribs.
- Symptoms that may worsen with twisting, bending, or prolonged sitting.
Lumbar Region (Low Back and Leg)
- Low back discomfort with radiating pain into the buttock, thigh, calf, or foot.
- Tingling or numbness along the leg in a narrow strip.
- Weakness lifting the foot, climbing stairs, or pushing off with the toes.
- Classic sciatic-type leg pain when lower lumbar roots are involved.
⚡ Sciatica (Shooting or Burning Leg Pain)
🧠 Radicular Pain (Pinched Nerve)
👣 Walking-Related Leg Pain (Claudication)
🍑 Sciatica vs Piriformis Syndrome
Other conditions such as disc herniation without nerve involvement, spinal instability, vertebrogenic pain, or hip and sacroiliac problems can mimic nerve-root patterns. A careful evaluation helps distinguish among these possibilities.
Radiculopathy, “Pinched Nerve,” and Sciatica: How They Relate
Patients often hear different terms from different providers. They are related but not identical:
- Radiculopathy: A problem affecting the spinal nerve root as it exits the spine, causing arm or leg symptoms.
- Pinched nerve root: A common way to describe the same process; see our detailed pinched nerve root discussion.
- Sciatica: Radiating leg pain from lower lumbar nerve-root irritation, usually from levels that contribute to the sciatic nerve; see our dedicated sciatica page.
You do not necessarily have three separate conditions. These terms often describe different aspects of the same underlying issue.
How We Distinguish Radiculopathy From Similar Conditions
Many problems can cause arm or leg symptoms. One key goal of your visit is separating true nerve-root irritation from “mimics.”
- Radiculopathy (nerve root): Symptoms often follow a narrow, predictable path (a dermatome/myotome pattern). The exam may show changes in strength, reflexes, or sensation. Certain spine positions may reproduce symptoms.
- Peripheral nerve entrapment (e.g., carpal tunnel, ulnar neuropathy): Symptoms follow a single peripheral nerve distribution rather than a root pattern and may be triggered by local pressure or repetitive use.
- Peripheral neuropathy: Often more diffuse and sometimes symmetric (for example, “stocking-glove” numbness), rather than one clear root pathway.
- Myofascial or joint-related pain: Can refer pain into an arm or leg, but usually without consistent dermatomal numbness or objective neurologic deficits.
- Hip, sacroiliac, or vascular causes: May mimic leg symptoms and need to be considered—especially when symptoms are activity- or walking-related.
In complex cases, Dr. Sharma may recommend electrodiagnostic testing (EMG and nerve conduction studies) to help distinguish nerve-root involvement from other nerve problems.
How Dr. Sharma Evaluates Nerve-Root Related Symptoms
A precise diagnosis is the foundation of effective care. During your visit, Dr. Sharma typically:
- Listens carefully to your story – how symptoms began, what worsens or eases them, and how they affect work, family, and day-to-day life.
- Performs a detailed neurologic and spine exam – checking strength, reflexes, sensation, and specific movements that may reproduce symptoms.
- Reviews or orders imaging when appropriate – such as MRI or CT scans to evaluate discs, joints, and nerve-root spaces.
- Considers electrodiagnostic testing – such as EMG and nerve conduction studies in complex cases, to help distinguish nerve-root involvement from other nerve problems.
The goal is to match your symptoms and exam findings with imaging, not to treat the scan in isolation. This approach helps avoid unnecessary procedures and focuses treatment on the structures most likely responsible for your symptoms.
How Long Does Radiculopathy Usually Last?
Many people improve over time, but recovery depends on what is irritating the nerve root, how long symptoms have been present, and whether there is numbness or weakness.
- Milder cases often improve over weeks as inflammation settles.
- Disc-related irritation can take 6–12 weeks (or longer) to calm down, especially if symptoms flare with activity.
- Numbness or weakness may improve more slowly than pain and deserves monitoring.
- Worsening weakness, walking difficulty, or bowel/bladder changes should be evaluated promptly rather than “waiting it out.”
Treatment Options for Radicular Nerve Symptoms
Treatment is individualized and usually follows a stepwise, minimally invasive strategy tailored to your goals and overall health.
Step 1: Conservative Care
- Activity modification: Adjusting lifting, posture, or repetitive movements that aggravate symptoms.
- Targeted physical therapy: Emphasizing posture, core and neck stabilization, flexibility, and nerve-mobilization techniques.
- Medications when appropriate: Short-term use of anti-inflammatory medicines, nerve-calming agents, or muscle relaxants.
- Home exercise programs: Supporting long-term spine health, rather than relying only on passive treatments.
Step 2: Image-Guided Procedures
If symptoms persist despite a well-designed conservative plan, image-guided procedures can directly target inflamed or compressed nerve roots. Depending on your specific pattern, Dr. Sharma may discuss:
- Selective nerve-root blocks: Precisely targeted injections around a single nerve root to reduce inflammation and clarify the pain source.
- Epidural steroid injections: Delivered under fluoroscopic guidance in the neck or low back to calm irritated nerve roots and create a window for rehabilitation.
- Facet or joint-directed procedures: When arthritic joints contribute to narrowing around the nerve root.
- Other minimally invasive options: Tailored to your anatomy and clinical picture, with the goal of avoiding large incisions whenever possible.
Step 3: When Are Advanced Procedures or Surgery Considered?
Many people with nerve-root related symptoms never require major open spine surgery. However, additional intervention may be appropriate when:
- Severe symptoms persist despite a thoughtful course of conservative and minimally invasive care.
- There is significant or progressive weakness in the arm or leg.
- Imaging shows clear structural compression of a nerve root that is unlikely to improve without intervention.
In these situations, treatment does not automatically mean “big surgery.” Depending on the cause, location, and stability of the problem, Dr. Sharma may discuss **advanced minimally invasive or motion-preserving options** designed to directly relieve nerve-root compression while limiting tissue disruption.
These may include:
- Endoscopic discectomy: A targeted, camera-assisted approach to remove disc material pressing on a nerve root through very small incisions.
- Disc-Fx and percutaneous disc procedures: Minimally invasive techniques that decompress or modify disc material contributing to nerve irritation in selected patients.
- Interspinous or stabilization devices (such as InSpan): Motion-preserving options used in carefully selected cases to address nerve compression related to segmental instability.
When appropriate, Dr. Sharma can perform or coordinate these advanced procedures and, if necessary, facilitate referral to spine surgeons who specialize in the **least invasive effective approach** for your specific condition.
Dr. Amit Sharma & our minimally invasive pain & spine team.
When Symptoms Need Urgent Attention
Most nerve-root related symptoms are painful and disruptive but not immediately dangerous. Certain features, however, warrant prompt or emergency evaluation:
- Sudden or rapidly worsening weakness in an arm or leg.
- Loss of control of bowel or bladder function.
- Numbness in the groin or “saddle” region.
- Severe, unrelenting pain combined with fever, chills, or unexplained weight loss.
If you are unsure whether your symptoms could represent an emergency, seek immediate medical care rather than waiting for a routine appointment.
Why Choose Dr. Amit Sharma for Nerve-Root Related Pain on Long Island?
- Advanced training: Johns Hopkins–trained interventional spine and pain specialist with extensive experience in image-guided and minimally invasive spine procedures.
- Minimally invasive and motion-preserving focus: Emphasis on office-based, percutaneous, and advanced targeted procedures designed to relieve nerve-root compression while helping many patients avoid major open surgery.
- Comprehensive decision-making: Evaluation of discs, joints, muscles, stability, and nerve structures together—not just a single MRI finding—to identify the true pain generator.
- Thoughtful escalation of care: Expertise in guiding patients from conservative treatment through advanced minimally invasive options, with surgical referral reserved for situations where it is truly necessary.
- Local access: Multiple convenient Long Island locations, including Bay Shore, Bethpage, Commack, and other nearby communities in Nassau and Suffolk counties.
- Personalized plans: Treatment built around each patient’s goals, work demands, neurologic findings, and overall health.
Nerve-root related arm or leg symptoms can be frightening, especially when they involve weakness or persistent numbness. A thoughtful, evidence-guided approach—focused on accurate diagnosis, appropriate intervention, and preservation of function—can help calm the irritated nerve and support a safe return to the activities that matter to you.
Related Conditions We Treat
- Sciatica and leg pain
- Sciatica vs radicular leg pain
- Pinched nerve root
- Herniated disc pain
- Spinal instability
- Vertebrogenic low back pain
- Cervicobrachial pain syndromes
Dr. Amit Sharma & our minimally invasive pain & spine team.
Radiculopathy FAQs
Is this the same thing as sciatica?
Not always. “Sciatica” refers specifically to radiating leg pain from lower lumbar nerve-root involvement. Nerve-root irritation higher in the lumbar spine, in the neck, or in the mid-back produces different patterns but is still considered a form of radicular nerve-root problem.
Can these symptoms improve on their own?
Yes. Many people experience gradual improvement over weeks to months as inflammation settles and the body adapts. However, persistent, severe, or progressive symptoms – especially weakness – should be evaluated so that important problems are not missed.
Do I always need an MRI right away?
Imaging decisions depend on how long symptoms have been present, their severity, and whether worrisome signs such as progressive weakness or bowel/bladder changes are present. In some cases, a careful exam and a short trial of conservative care may be reasonable before ordering advanced imaging.
Is radicular nerve pain dangerous?
In most cases it is not life-threatening, but it can significantly affect quality of life and function. Sudden weakness, difficulty walking, or bowel/bladder changes are more urgent and deserve immediate attention.
What Is the “Best” Treatment?
The best approach depends on the specific nerve root involved, what is compressing or irritating it, how long symptoms have been present, and your overall health and goals.
Many patients improve with a combination of targeted physical therapy, activity modification, medications when appropriate, and image-guided procedures to calm nerve inflammation and support recovery.
When symptoms persist or neurologic deficits develop, treatment does not automatically mean major open surgery. In selected cases, advanced minimally invasive or motion-preserving procedures may be appropriate to directly relieve nerve-root compression while limiting tissue disruption. Surgery is reserved for situations where less invasive options are unlikely to provide adequate relief or protection of nerve function.
For more background, you can review patient education from Johns Hopkins Medicine, the Cleveland Clinic, Mayo Clinic, or peer-reviewed resources such as Spine-health.
- Radiculopathy overview – Johns Hopkins Medicine
- Radiculopathy: Symptoms, Causes & Treatment – Cleveland Clinic
- Radiculopathy – Mayo Clinic Orthopedics & Sports Medicine
- Cervical radiculopathy symptoms – Spine-health
This page is for educational purposes only and is not a substitute for personal medical advice, diagnosis, or treatment. For an individualized assessment and treatment plan, please schedule a consultation.



