Maigne Syndrome: 7 Key Signs of Overlooked Back Pain
Many people live with chronic low back, buttock, or “hip” pain even after an MRI, physical therapy, and the usual treatments. When the story doesn’t add up, an often-missed diagnosis called Maigne syndrome may be the missing puzzle piece.
Maigne syndrome (also called thoracolumbar junction syndrome) is a pattern of referred pain that starts higher in the spine (usually around T12–L2) and “projects” discomfort to areas such as the top of the pelvis (iliac crest), upper buttock, lateral hip, groin, or lower abdomen. Because the pain shows up away from the true source, it is commonly mistaken for sacroiliac joint pain, lumbar disc problems, or hip disease.
If you’re trying to understand where your pain may be coming from, you can also use our Pain Locator to match your symptoms with common (and uncommon) pain generators.
What Is Maigne Syndrome?
Maigne syndrome describes pain caused by irritation or dysfunction at the thoracolumbar junction, the transition zone where the lower thoracic spine meets the upper lumbar spine. This area is a biomechanical “border crossing” where the spine shifts its movement patterns, making it vulnerable to overload and irritation.
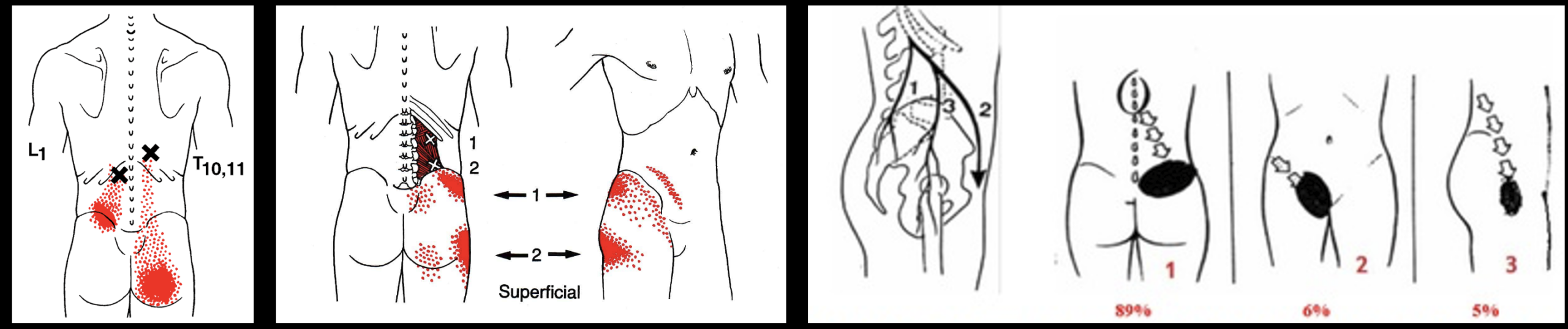
The hallmark feature is referred pain mediated by nerve branches that can trigger pain in predictable regions. The most discussed pathway involves sensory nerves that contribute to the superior cluneal nerves, which travel over the back of the pelvis and supply sensation to the upper buttock and iliac crest. When those nerve inputs are irritated near their spinal origin, pain can be felt along the pelvis and buttock instead of (or in addition to) the spine itself.
For a deeper medical overview, see: Maigne Syndrome – a potentially treatable yet often unrecognized cause of low back pain (PubMed) and Thoracolumbar junction syndrome clinical presentation (PMC).
Why Maigne Syndrome Is Frequently Missed
- Imaging often doesn’t “explain” the pain. Lumbar MRIs may show mild bulges or age-related changes that don’t match symptom severity, and the thoracolumbar junction may not be the focus.
- Symptoms mimic common diagnoses. It can look like SI joint pain, facet pain, hip pathology, or “muscle” pain.
- The pain location is misleading. Patients often point to the pelvis, buttock, or side of the hip, not the spine.
- It’s under-taught. Many clinicians rarely discuss Maigne syndrome explicitly, so it doesn’t get considered early.
If your symptoms overlap with common categories, you may also find these guides helpful: Back Pain, Leg Pain, Neck Pain, and our overview on Spine Pain.
Maigne Syndrome: 7 Key Signs of Overlooked Back Pain
1) Pain Over the Top of the Pelvis (Iliac Crest Pain)
A classic clue is pain and tenderness along the iliac crest, often toward the back portion. Patients may describe:
- “Pain right along the top of my hip bone.”
- Local sensitivity to touch over the pelvic rim.
- Discomfort when wearing belts or tighter waistbands.
2) Pain That Wraps From the Low Back to the Side of the Hip
Instead of centered (midline) back pain, symptoms may feel like they “wrap” outward toward the upper buttock or lateral hip. This is a common referred-pain pattern and can be confused with a hip problem even when the hip joint is normal.
3) MRI Findings That Don’t Match the Intensity of Symptoms
Many people with Maigne syndrome have a lumbar MRI that reads “mild degenerative changes” or “small disc bulge,” but the symptoms feel far more disruptive than expected. When imaging and real-life pain don’t match, it’s a sign the pain generator may be overlooked.
4) Worse With Standing, Walking, or Extension
Symptoms often worsen with:
- Prolonged standing
- Walking longer distances
- Arching backward (extension)
- Twisting through the trunk
This can mimic SI joint or facet pain, but the thoracolumbar junction is the upstream culprit in Maigne syndrome.
5) Tenderness Near the Thoracolumbar Junction (T12–L2)
On exam, a clinician may reproduce symptoms by pressing just off the midline near the thoracolumbar junction. This may reflect irritation in facet joints or surrounding structures contributing to referred pain.
6) Upper Buttock Pain Without True Sciatica
Maigne-related pain often stays above the knee and does not behave like classic lumbar radiculopathy (true sciatica). Many patients have buttock pain but lack:
- Clear numbness/tingling down a specific nerve-root path
- Weakness in the foot/ankle
- Pain reliably traveling below the knee
7) Meaningful Relief From Targeted Diagnostic Blocks
One of the strongest clues is improvement after a precise diagnostic injection targeting the suspected pain generator. If a properly placed block provides clear, immediate relief, it helps confirm the diagnosis and guides next-step treatment.
Related reading on cluneal nerve pain patterns: Superior cluneal nerve entrapment syndrome overview (PMC) and Superior cluneal neuralgia as an underappreciated cause of low back pain (PMC).
Maigne Syndrome vs. SI Joint Pain vs. Disc Pain
Maigne Syndrome vs. Sacroiliac Joint Pain
- SI joint pain often feels deeper and lower near the buttock dimples and may worsen with specific SI stress tests.
- Maigne syndrome often features iliac crest tenderness and pain that feels like it “rides the rim” of the pelvis.
- If SI injections help only partially or briefly, the thoracolumbar junction may be a missed source.
Maigne Syndrome vs. Lumbar Disc Herniation
- Disc herniation more often causes radiating leg pain below the knee with numbness/tingling and possible weakness.
- Maigne syndrome more often stays in the low back, iliac crest, upper buttock, hip, or groin region without a classic nerve-root pattern.
If your main symptom is radiating leg pain, see our guide on Leg Pain.
How Maigne Syndrome Is Diagnosed
Diagnosis is typically based on a combination of the clinical pattern and response to targeted treatment. The process often includes:
- History: pain location (iliac crest/upper buttock), triggers (standing/extension), and what has not worked so far.
- Physical exam: tenderness patterns, movement-provoked pain, and specific palpation findings near the thoracolumbar junction and iliac crest.
- Diagnostic blocks: image-guided injections to confirm the pain source when appropriate.
For clinicians and medically-inclined readers, additional references include: <ahref=”https://pubmed.ncbi.nlm.nih.gov/39692376/” target=”_blank” rel=”noopener”>Maigne’s thoracolumbar junction syndrome summary (PubMed) and Exercise vs. local steroid injection outcomes in TLJ syndrome (PMC).
Treatment Options for Maigne Syndrome
Targeted Physical Therapy and Mobility Work
Therapy aims to reduce mechanical stress at the thoracolumbar junction and improve control through the core and thoracolumbar region. A generic “low back PT” plan may not be enough. The best results come from identifying the movement patterns that aggravate the junction and correcting them.
Anti-inflammatory and Symptom Management
Medication may help reduce pain flares, but it usually does not address the mechanics that keep the thoracolumbar junction irritated.
Image-guided Injections
Depending on the clinical pattern, options may include targeted blocks to confirm and treat the pain generator. These injections can be both diagnostic and therapeutic.
Radiofrequency Ablation
If diagnostic blocks provide strong but temporary relief, radiofrequency ablation may be considered in carefully selected cases to provide longer-lasting improvement.
To explore your interventional options and understand common pain generators, visit: Spine Pain and our symptom-based Pain Locator.
When to Consider an Expert Evaluation
Consider evaluation for Maigne syndrome if you have:
- Pain along the top of the pelvis (iliac crest) or upper buttock
- “Hip pain” but normal hip imaging or exam
- A lumbar MRI that doesn’t explain the severity of symptoms
- Incomplete relief after standard back or SI joint treatments
- Pain worse with standing, walking, extension, or twisting
If you’re ready to pinpoint the cause and match symptoms to likely pain generators, start here: Pain Locator.
Frequently Asked Questions
Is Maigne syndrome serious?
It’s typically not “dangerous,” but it can be highly disruptive and stubborn when overlooked. The main risk is prolonged suffering from missed diagnosis and misdirected treatment.
Can Maigne syndrome cause groin or abdominal pain?
Yes. Referred pain from the thoracolumbar junction can present as pseudo-visceral pain in the groin or lower abdomen in some patients.
Does it always show on MRI?
No. Many patients have normal or only mildly abnormal imaging. Diagnosis is often clinical and may be supported by targeted diagnostic blocks.
References
- Karl HW, Helm S, Trescot AM. Superior and Middle Cluneal Nerve Entrapment: A Cause of Low Back and Radicular Pain. Pain Physician. 2022 Jul;25(4):E503-E521. PMID: 35793175.
- Talu GK, Ozyalçin S, Talu U. Superior cluneal nerve entrapment. Reg Anesth Pain Med. 2000 Nov-Dec;25(6):648-50. doi: 10.1053/rapm.2000.18189. PMID: 11097676.
- Karri J, Singh M, Orhurhu V, Joshi M, Abd-Elsayed A. Pain Syndromes Secondary to Cluneal Nerve Entrapment. Curr Pain Headache Rep. 2020 Aug 21;24(10):61. doi: 10.1007/s11916-020-00891-7. PMID: 32821979.
Dr. Amit Sharma & our minimally invasive pain & spine team.
Medical Disclaimer: This article is for education only and does not provide medical advice. A proper diagnosis requires an in-person evaluation and appropriate testing. If you have severe or progressive weakness, bowel/bladder changes, fever, unexplained weight loss, or significant trauma, seek urgent medical care.



