
Degenerative Disc Disease: Causes, Symptoms & Treatment Options
Degenerative Disc Disease (DDD) is one of the most common causes of chronic back and neck pain, yet it remains widely misunderstood. Despite its name, DDD is not technically a disease but a natural part of aging that can, in some cases, lead to debilitating symptoms. Understanding this condition is crucial to managing pain and maintaining spinal health.
At SpinePain Solutions, Dr. Amit Sharma offers advanced treatments, including regenerative medicine, to help patients manage and overcome the challenges of Degenerative Disc Disease.
What is Degenerative Disc Disease (DDD)?
DDD refers to the gradual wear and tear of the intervertebral discs — the soft cushions that separate and protect your spinal vertebrae. Over time, these discs lose hydration and elasticity, reducing their ability to absorb shock. This process can lead to pain, reduced mobility, and in some cases, nerve compression.
While aging is the primary factor, not everyone will experience symptoms. For those who do, pain management and targeted therapies can significantly improve quality of life.
Cervical vs Lumbar Degenerative Disc Disease
Degenerative disc disease can affect both the neck and the lower back, but the symptoms and treatment pathways are often different.
Cervical Degenerative Disc Disease
When disc degeneration occurs in the neck, patients may experience neck stiffness, shoulder blade pain, headaches, or pain that travels into the arm. If a cervical nerve root becomes irritated or compressed, symptoms may include numbness, tingling, or weakness. Learn more about related symptoms on our pages about neck pain, cervicobrachial pain, and cervical radiculopathy.
Lumbar Degenerative Disc Disease
When disc degeneration occurs in the lower back, patients often describe deep low back pain that may worsen with sitting, bending, lifting, or prolonged activity. In some cases, disc degeneration can contribute to nerve irritation, sciatica, spinal stenosis, or vertebrogenic pain. Learn more about back pain, sciatica, and vertebrogenic pain.
Key Risk Factors for DDD
Although disc degeneration is a natural part of aging, certain lifestyle and genetic factors increase the risk of developing symptomatic Degenerative Disc Disease. These include:
- Repetitive heavy lifting or physical labor
- Obesity, which places excess stress on the spine
- Smoking, which impairs disc nutrition
- Previous spinal injuries or trauma
- Genetic predisposition to early disc degeneration
Studies, such as those from PubMed, confirm that lifestyle modifications can slow the progression of disc degeneration.
Recognizing Symptoms of DDD
Many individuals with Degenerative Disc Disease remain asymptomatic. However, when symptoms occur, they typically include:
- Centralized low back or neck pain
- Pain that worsens with sitting, bending, or lifting
- Relief when walking, standing, or lying down
- Occasional radiating pain to the buttocks or thighs (but rarely below the knee)
This type of discomfort is known as discogenic pain. It arises directly from the damaged disc rather than nerve root compression.
Diagnosing Degenerative Disc Disease: Facing the 800-Pound Gorilla
Accurately diagnosing Degenerative Disc Disease (DDD) is both an art and a science. It requires a thoughtful combination of detailed medical history, comprehensive physical examination, and advanced imaging techniques like MRI or CT scans. But here’s the challenge — while imaging can reveal disc degeneration, these findings are often present in people who have no back pain at all.
This disconnect between what we see on scans and what patients feel makes diagnosing discogenic pain far more complex than simply pointing to a degenerated disc on an MRI. In certain nuanced cases, tools like provocative discography have been used in an attempt to pinpoint the exact source of pain, particularly when multiple degenerated discs are visible. However, even these approaches come with controversy and limitations.
We could easily turn this discussion into an entire textbook chapter — but it’s impossible to ignore the central question every patient and clinician faces when dealing with chronic back pain:
“How do we truly determine if your back pain is coming from Degenerative Disc Disease?”
Discogenic Vs.Vertebrogenic Pain
Although they may sound similar, discogenic pain and vertebrogenic pain are not the same. Understanding their differences is essential for accurate diagnosis and treatment planning. There is an overlap between this article and the the vertebrogenic pain article.
🔹 Discogenic Pain
Discogenic pain arises from the intervertebral disc itself, particularly the outer annulus fibrosus, which is innervated by the sinuvertebral nerve. This type of pain is often triggered by:
- Annular fissures or internal disc disruption
- High-intensity zones (HIZ) on MRI
- Intradiscal pressure (e.g., sitting, forward flexion)

HIZ |
 |
🔹 Vertebrogenic Pain
Vertebrogenic pain is a more specific clinical diagnosis that refers to chronic low back pain originating from endplate damage and inflammation, mediated by the basivertebral nerve (BVN).
Key features include:
- Presence of Modic type 1 or 2 changes on MRI
- Inflammation at the vertebral endplates
- Not caused by disc herniation, facet joints, or sacroiliac joints
This condition is often treated with the Intracept Procedure, which involves radiofrequency ablation of the BVN.
Unlike vertebrogenic pain, discogenic pain may be confirmed by provocative discography (controversial issue) and is typically addressed using regenerative therapies (e.g., PRP, stem cells) or intradiscal electrothermal therapy (IDET), or biacuplasty.
🔹 Key Anatomical Differences
| Feature | Discogenic Pain | Vertebrogenic Pain |
|---|---|---|
| Source | Annulus fibrosus | Vertebral endplates |
| Nerve Pathway | Sinuvertebral nerve | Basivertebral nerve (BVN) |
| Typical Imaging | High-intensity zone, annular tear | Modic type 1 or 2 changes |
| Symptoms | Axial pain worsened by sitting, flexion | Deep midline pain, prolonged standing, activity |
| Treatment | Regenerative (PRP, stem cells), IDET | Intracept Procedure (BVN ablation) |
✅ Clarifying Statement
💡 Clinical Pearl: While both discogenic and vertebrogenic pain stem from degenerative spinal changes, they are distinct entities with different anatomical origins, neural pathways, and treatment strategies. Accurate differentiation is essential for optimal care.
Stages of Degenerative Disc Disease and Endplate Involvement
Degenerative Disc Disease (DDD) is a progressive condition in which intervertebral discs lose hydration, elasticity, and structural integrity over time. This degeneration places increased stress on adjacent vertebral endplates, often contributing to vertebrogenic pain.
Common Stages of DDD Progression:
- Stage 1 – Early Disc Dehydration: Nucleus pulposus begins to lose water content. MRI shows mildly decreased T2 signal. Patients may have little or no symptoms.
- Stage 2 – Disc Narrowing and Annular Fissures: Disc height starts to reduce. Small annular tears may develop. Endplates show signs of early stress and inflammation.
- Stage 3 – Advanced Degeneration: Disc collapses. There is significant loss of height and signal. Endplates appear sclerotic or eroded. This stage is commonly associated with Modic changes and vertebrogenic pain.
- Stage 4 – Segmental Instability and Facet Arthropathy: Severe disc collapse causes abnormal motion and facet joint overload. May lead to stenosis and nerve root involvement.
Modified Pfirrmann Grading Scale (Grades 1–8)
The Modified Pfirrmann Scale is a widely used MRI grading system for lumbar disc degeneration. It assesses disc hydration, signal intensity, structure, and disc height. A modified classification was proposed in 2007 by Griffith et al. to better categorize degenerative discs in older patients where most discs are Pfirrmann grade III or IV. It has, however, not been as widely adopted.
| Grade | T2 Signal Intensity | Annular Fiber Junction | Disc Height |
|---|---|---|---|
| Grade 1 | Uniformly hyperintense, equal to CSF | Distinct junction between inner and outer annular fibers posteriorly | Normal |
| Grade 2 | Hyperintense (between presacral fat and CSF), ± hypointense intranuclear cleft | Distinct junction | Normal |
| Grade 3 | Hyperintense (less than presacral fat) | Distinct junction | Normal |
| Grade 4 | Mildly hyperintense (slightly more than outer annular fibers) | Indistinct junction | Normal |
| Grade 5 | Hypointense (equal to outer annular fibers) | Indistinct junction | Normal |
| Grade 6 | Hypointense | Indistinct junction | ~30% reduction |
| Grade 7 | Hypointense | Indistinct junction | 30–60% reduction |
| Grade 8 | Hypointense | Indistinct junction | >60% reduction |

Integration into Clinical Decision-Making
Recognizing whether a patient’s axial pain is discogenic or vertebrogenic helps guide the therapeutic approach:
- Stages 2–5 Pfirrmann: More favorable for regenerative intradiscal therapy
- Stages 6–8 Pfirrmann: Often associated with Modic changes and vertebrogenic pain → Intracept is more appropriate
Self-Assessment Scoring Tool
This simple point-based system helps non-specialists gauge whether their low back pain may be discogenic or vertebrogenic in origin. While not diagnostic, it can encourage appropriate next steps:
- 1 point: Persistent midline low back pain (axial)
- 1 point: Absence of radicular pain or sciatica extending past the knee (learn more)
- 1 point: Pain duration >3 months
- 1 point: Pain worsens while sitting
- 1 point: Pain worsens during forward flexion
- 1 point: Pain improves with standing
- 1 point: MRI shows Modic changes (Type 1 or 2)
- 1 point: MRI shows high-intensity zones or annular tears
- 1 point: Facet joint syndrome ruled out via diagnostic medial branch block
- 1 point: SI joint dysfunction ruled out via diagnostic SI joint injection
Interpretation:
- 0–4 points: Low probability — conservative care may be sufficient
- 5–7 points: Moderate probability — likely structural pain generator; clinical imaging and expert evaluation recommended
- 8–10 points: High probability — strong candidate for advanced diagnostic workup, including targeted image-guided injections
Note: This tool is an educational guide and not a substitute for formal clinical diagnosis. Accurate evaluation requires high-quality spine MRI, physical examination, and expert correlation using validated diagnostic techniques.
📞 Ready to Take the Next Step?
If your symptoms align with the scoring criteria above, or if you’re seeking expert evaluation for persistent back pain, schedule a consultation with Dr. Amit Sharma.
Potential Complications
Advanced Degenerative Disc Disease can lead to complications such as:
- Spinal osteoarthritis
- Disc herniation
- Spinal stenosis
- Formation of bone spurs
These conditions may exacerbate pain and neurological symptoms, requiring more specialized interventions.
Effective Treatment Options for DDD
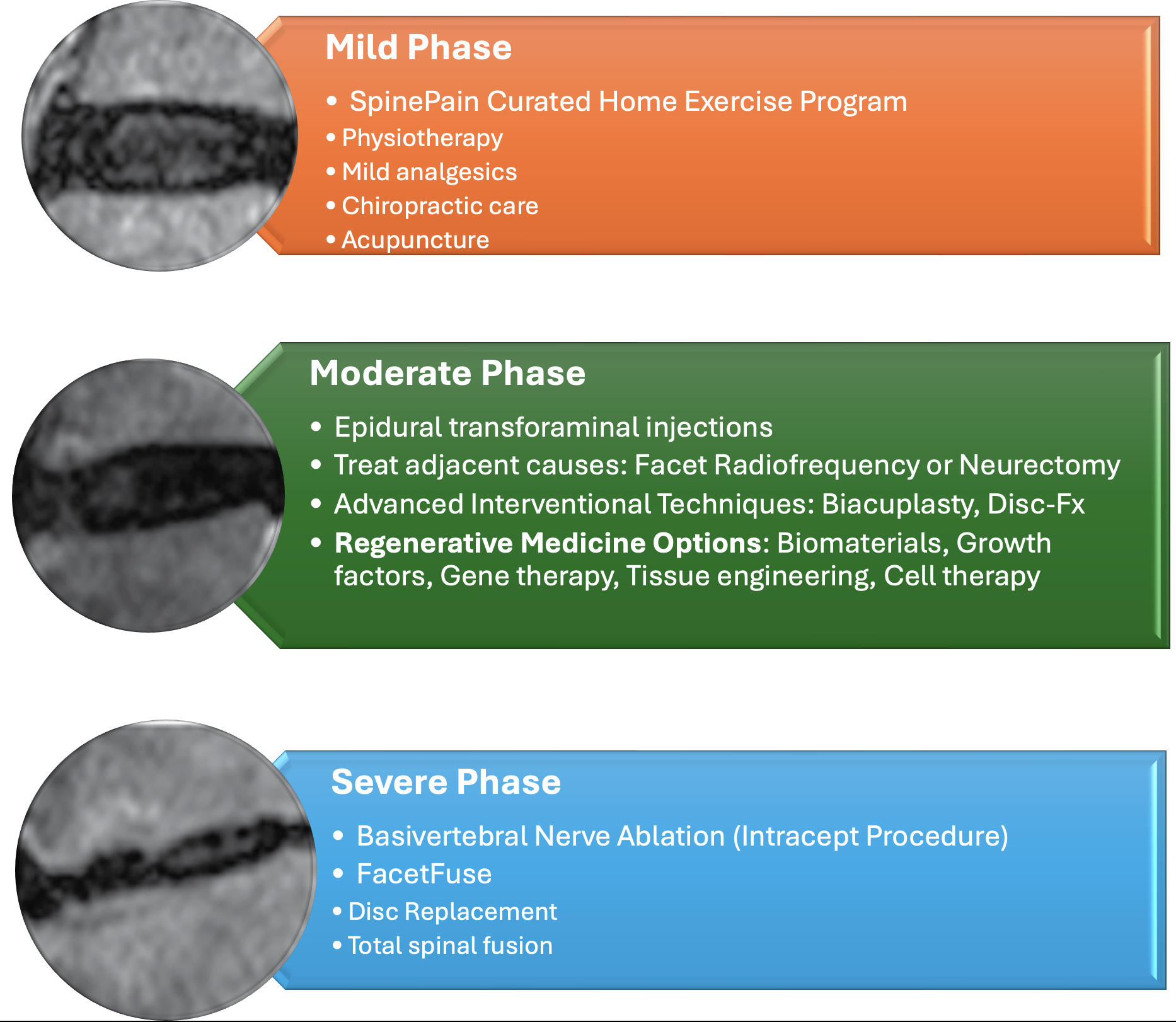
Most cases of Degenerative Disc Disease are managed conservatively. Initial treatments include:
- A curated self help home based exercise program (SpinePain HEP) and core strengthening
- Formal Physical therapy
- Chiropractic care or acupuncture
- Anti-inflammatory medications
When to Consider Advanced Treatments for DDD
When conservative treatments fail to control symptoms of Degenerative Disc Disease after 2 months, it may be time to explore advanced, minimally invasive options. Chronic discogenic pain can interfere with daily life, but interventional procedures offer targeted relief without the need for major surgery. Dr. Amit Sharma provides specialized treatments designed to reduce pain, restore function, and delay or prevent surgical intervention.
Why Choose Interventional Treatments?
Persistent pain from Degenerative Disc Disease often results from inflammation, nerve irritation, or biomechanical instability. Interventional procedures address these issues by:
- Decreasing inflammation around spinal nerves
- Interrupting pain signals from degenerated discs
- Supporting structural integrity through biologic therapies
- Promoting long-term spine health
Interventional Options Offered by Dr. Sharma
Epidural Steroid Injections (Interlaminar Approach))
ESI reduces inflammation around compressed nerves, providing temporary pain relief and allowing patients to participate in rehabilitation. It’s typically recommended when nerve-related leg or arm pain accompanies disc degeneration.
Epidural Steroid Injections (Transforaminal Approach)
When it comes to managing nerve-related pain from Degenerative Disc Disease, not all epidural steroid injections (ESIs) are created equal. Dr. Sharma specializes in the Transforaminal Epidural Steroid Injection (TFESI), a targeted technique proven to deliver superior outcomes compared to traditional approaches.
Why Transforaminal Injections Are Superior:
- Precise Delivery: TFESI allows the anti-inflammatory steroid to be placed directly at the site where the nerve exits the spine (the foramen), ensuring maximum impact on the irritated nerve root.
- Better Pain Relief: Studies have shown that transforaminal injections provide more effective and longer-lasting relief for radicular pain (sciatica) than interlaminar or caudal approaches.
- Lower Medication Volume, Higher Efficacy: Because of its precision, TFESI requires a smaller dose of steroid while achieving better therapeutic outcomes, reducing systemic side effects.
- Diagnostic Advantage: TFESI can also help confirm which specific nerve root is causing symptoms, guiding further treatment decisions.
When is TFESI Recommended?
Dr. Sharma recommends transforaminal injections for patients experiencing leg or arm pain due to nerve compression from disc degeneration or disc herniation. It’s especially useful when conservative treatments have failed, but surgery is not yet warranted. By choosing TFESI, patients benefit from a precise, minimally invasive solution that addresses the root cause of their nerve pain associated with Degenerative Disc Disease.
Intradiscal Biacuplasty
This procedure uses radiofrequency energy to target nerves within a painful disc, reducing chronic discogenic pain without affecting surrounding tissues. Ideal for patients with confirmed disc pain unresponsive to conservative care.
ViaDisc Allograft
A regenerative therapy where biologic material is injected into the degenerated disc to restore hydration and cushioning. This innovative approach addresses the underlying cause of Degenerative Disc Disease.
Intracept Procedure
Targets the basivertebral nerve inside the vertebrae responsible for transmitting chronic low back pain signals related to vertebral and disc degeneration.
Regenerative Medicine Therapies
Dr. Sharma integrates advanced regenerative medicine techniques to treat DDD. These biologic treatments aim to heal, not just mask symptoms, making them ideal for patients seeking non-surgical solutions to Degenerative Disc Disease.
Intradiscal Regenerative Medicine Options for Degenerative Disc Disease
Emerging regenerative therapies offer promising alternatives to traditional treatments for Degenerative Disc Disease (DDD). Below is a comparison of three notable intradiscal regenerative options.
1. Platelet-Rich Plasma (PRP)
Overview: PRP involves concentrating a patient’s own platelets and injecting them into the degenerated disc to promote healing.
Evidence: A study demonstrated significant pain relief and improved lumbar function over a 48-week period following intradiscal PRP injections. [Study Link]
2. Bone Marrow Concentrate (BMC)
Overview: BMC is derived from the patient’s own bone marrow and contains stem cells and growth factors that may aid in disc regeneration.
Evidence: Research indicates that intradiscal BMC injections can lead to significant improvements in pain and disability scores, with sustained benefits observed over a three-year follow-up. [Study Link]
3. Wharton’s Jelly Mesenchymal Stem Cells (WJ-MSCs)
Overview: WJ-MSCs are derived from the gelatinous substance within the umbilical cord and have shown potential in regenerating degenerated discs.
Evidence: Animal studies suggest that WJ-MSC transplantation can maintain disc height and promote matrix formation, indicating their value in treating DDD. [Study 1 Link] [Study 2 Link]
Comparison Summary
| Therapy | Source | Key Benefits | Clinical Evidence |
|---|---|---|---|
| PRP | Autologous Blood | Reduces inflammation, promotes healing | Positive outcomes over 48 weeks |
| BMC | Autologous Bone Marrow | Contains stem cells, supports regeneration | Improved pain and function over 3 years |
| WJ-MSCs | Umbilical Cord Tissue | High proliferation, potential for disc repair | Maintained disc height and matrix formation |
FDA Disclaimer: The regenerative therapies discussed are considered investigational and are not yet approved by the U.S. Food and Drug Administration (FDA) for the treatment of Degenerative Disc Disease. Patients should consult with their healthcare providers to understand the potential risks and benefits.
💡 Want to Learn About Healing Your Spine?
Discover 7 proven regenerative solutions for disc repair—including stem cells, exosomes, and bioprinted discs—designed to restore structure and relieve pain without fusion surgery.
When is Surgery Considered?
We wish the answer is “never”, but it is far from the truth. Surgical intervention, like spinal fusion, is a last resort and generally avoided unless neurological deficits or severe instability occur. Let’s dig into this topic here:
Is Spinal Fusion a Permanent Solution for Degenerative Disc Disease?
Spinal fusion is often considered when severe Degenerative Disc Disease (DDD) leads to chronic pain unresponsive to other treatments. While fusion can reduce pain by eliminating motion at the degenerated segment, it is important to understand that it does not reverse disc degeneration or “cure” DDD.
Does It Get Better Forever?
For some patients, spinal fusion provides long-term pain relief. However, fusion alters spinal mechanics, often leading to a condition known as Adjacent Segment Disease (ASD), where discs above or below the fused segment begin to degenerate due to increased stress. Therefore, while spinal fusion may improve symptoms at one level, it can predispose patients to future spine problems. It is not typically considered a “permanent fix” for the spine overall.
The United States and Spinal Fusion Rates
The U.S. performs the highest number of spinal fusion surgeries worldwide. Studies show that spinal fusion rates in the U.S. have increased by over 300% in recent decades [Spine Journal]. Compared to countries like Sweden, the UK, or Canada—where stricter surgical criteria are applied—the U.S. healthcare system sees more frequent use of fusion, sometimes raising concerns about overuse.
Exploring the Future
As medical science evolves, new therapies are emerging that offer hope for patients suffering from Degenerative Disc Disease (DDD). Among these innovations, Hydrogel Injections are gaining attention as a minimally invasive solution aimed at restoring disc height and function.
Hydrogel Injections: Restoring Cushioning Within the Spine
What Are They? Hydrogel injections involve delivering a biocompatible, water-absorbing gel directly into the degenerated disc. This gel mimics the natural nucleus pulposus, helping to rehydrate the disc, restore its height, and improve shock absorption.
Clinical Promise: Early studies show that hydrogel implants can reduce pain and improve mobility by mechanically supporting the spine. One notable product under investigation is Hydrafil™, which has demonstrated encouraging outcomes in clinical trials.
Other Futuristic Treatments on the Horizon
- Gene Therapy: Researchers are exploring ways to modify gene expression within disc cells to slow or reverse degeneration. This could offer a biological repair mechanism at the molecular level.
- Tissue Engineering & 3D Bioprinting: Scientists are developing lab-grown disc tissues and scaffolds that could one day replace degenerated discs entirely.
- Exosome Therapy: Exosomes derived from stem cells are being studied for their ability to reduce inflammation and promote disc regeneration without introducing whole cells.
Where Do These Treatments Stand?
While these therapies are exciting, most remain in clinical trial phases or under regulatory review. However, they highlight a shift toward biologic and regenerative solutions that aim to repair rather than simply manage DDD.
Why Dr. Sharma Advocates for Non-Surgical Solutions First
Dr. Amit Sharma emphasizes motion-preserving, minimally invasive treatments for Degenerative Disc Disease. With advancements in regenerative medicine and interventional spine care, many patients can avoid the risks associated with spinal fusion. Procedures like Intradiscal Biacuplasty, ViaDisc Allograft, and biologic therapies (PRP, stem cells) offer effective alternatives focused on reducing pain, restoring function, and preserving spinal mobility.
Dr. Amit Sharma stays at the forefront of regenerative and interventional spine care. While many of these futuristic treatments are not yet widely available, Dr. Sharma offers current advanced options like ViaDisc Allograft, PRP, and stem cell therapies—bridging today’s care with tomorrow’s innovations. If back pain persists despite initial treatments, or if you’re looking for alternatives to surgery, schedule a consultation with Dr. Sharma to explore personalized interventional and regenerative options.
Take Control of Your Spine Health
If you’re struggling with chronic back pain and suspect Degenerative Disc Disease, early intervention can prevent progression. Contact Dr. Amit Sharma for a comprehensive evaluation and personalized treatment plan.
Frequently Asked Questions About Degenerative Disc Disease
Is Degenerative Disc Disease reversible?
No, but symptoms can be managed effectively with lifestyle changes, interventional procedures, and regenerative therapies.
What triggers flare-ups of Degenerative Disc Disease?
Flare-ups are often caused by prolonged sitting, poor posture, heavy lifting, repetitive bending, or lack of physical activity.
How is Degenerative Disc Disease diagnosed if imaging isn’t enough?
Diagnosis relies on a combination of symptom patterns, physical examination, selective imaging, and expert evaluation to rule out other causes.
Can Degenerative Disc Disease lead to long-term disability?
Severe, untreated cases can limit mobility, but early intervention significantly reduces this risk.
Is spinal fusion the only solution for Degenerative Disc Disease?
No, many patients benefit from non-surgical treatments like physical therapy, injections, and regenerative medicine before considering surgery.
How effective is regenerative medicine for Degenerative Disc Disease?
Emerging research supports PRP and stem cell therapies in reducing pain and improving disc function, though they remain investigational.
Is walking or exercise safe with Degenerative Disc Disease?
Yes, low-impact activities like walking can help maintain flexibility, strengthen core muscles, and reduce pain episodes.
Dr. Amit Sharma & our minimally invasive pain & spine team.
References
- Brinjikji et al., 2015 — MRI Findings in Asymptomatic Adults
- NIH: Discography in Lumbar Discogenic Pain
- PubMed: Differentiating Vertebrogenic and Discogenic Pain
- Spine Journal: The Economics of Spinal Fusion Surgery
- PubMed: Adjacent Segment Disease After Lumbar Fusion
- Global Spine Journal: International Trends in Spine Surgery
- PMC: Intradiscal PRP for Discogenic Low Back Pain
- PubMed: Bone Marrow Concentrate for Degenerative Disc Disease
- PMC: Wharton’s Jelly MSCs in Intervertebral Disc Regeneration
- PubMed: Hydrogel Injection for Intervertebral Disc Degeneration
- PMC: Exosome-Based Therapies in Spine Degeneration



