Lamina Pain Guide: 7 Critical Facts on Causes & Treatment
The lamina, a crucial component of vertebral anatomy, plays a significant role in protecting the spinal cord and providing structural support. However, various clinical conditions can affect this structure, leading to pain and functional impairments. This article explores the anatomy of the lamina, clinical conditions associated with it, diagnostic approaches, and interventional treatment options.
Anatomy of the Lamina
The lamina is a part of each vertebra in the spine, forming the posterior section of the vertebral arch. There are two laminae per vertebra, one on each side, which connect the spinous process to the transverse processes and pedicles. The primary functions include:
- Protecting the Spinal Cord: By forming part of the vertebral canal, it safeguards the spinal cord and nerve roots.
- Providing Structural Support: It contributes to the stability and integrity of the vertebral column.
- Attachment Points: Serves as a site for the attachment of muscles and ligaments that facilitate movement and maintain posture.
Clinical Conditions Related to the Lamina
Several conditions can affect the posterior vertebral elements and result in pain or neurological symptoms:
- Lamina Fractures: Often result from trauma, such as falls or accidents, and may cause acute pain and instability.
- Spondylolysis: A stress fracture in the pars interarticularis, the segment between the lamina and pedicle, which can lead to spondylolisthesis.
- Lamina-Associated Stenosis: Hypertrophy or thickening of the laminae may contribute to spinal stenosis, resulting in compression of the spinal cord or nerve roots.
- Osteoarthritis: Degenerative changes in the facet joints can affect adjacent posterior structures, leading to pain and reduced mobility.
- Tumors: Both benign and malignant growths may involve the lamina, causing pain, neurological deficits, or structural deformities.
Differential Diagnosis
Symptoms attributed to posterior vertebral structures may overlap with:
- Facet joint syndrome
- Discogenic pain
- Sacroiliac joint dysfunction
- Myofascial pain syndromes
- Radiculopathy from disc herniation
Work-Up and Diagnosis
A comprehensive work-up includes:
- Clinical Examination: Assessment of pain, range of motion, and neurological function.
- Imaging Studies:
- X-Rays: Initial assessment to identify fractures, alignment issues, and degenerative changes.
- MRI: Detailed imaging of soft tissues, including the spinal cord, nerve roots, and mass lesions.
- CT Scans: High-resolution visualization of bony anatomy, useful for detecting fractures and bony stenosis.
- Bone Scintigraphy: Identifies areas of increased metabolic activity related to fractures, tumors, or inflammation.
Red-Flag Symptoms
Seek urgent evaluation if pain is accompanied by:
- Progressive neurological weakness
- Loss of bowel or bladder control
- Saddle anesthesia
- Unexplained weight loss or night pain
- History of cancer, infection, or significant trauma
Treatment Options
Conservative treatments such as physical therapy, medications, and lifestyle modification are often first-line approaches. Interventional modalities play a critical role when symptoms persist or worsen.
Most patients experience improvement with conservative management over 6–12 weeks. Failure to respond, worsening pain, or neurological decline should prompt reconsideration of imaging or interventional referral.
Interventional Treatment Modalities
- Corticosteroid Injections: Targeted, image-guided injections around affected posterior elements or facet joints to reduce inflammation.
- Radiofrequency Ablation (RFA): A minimally invasive technique used to interrupt pain transmission from nerves supplying posterior spinal structures.
- Percutaneous Vertebroplasty or Kyphoplasty: Cement augmentation procedures used in select fracture cases to stabilize bone and relieve pain.
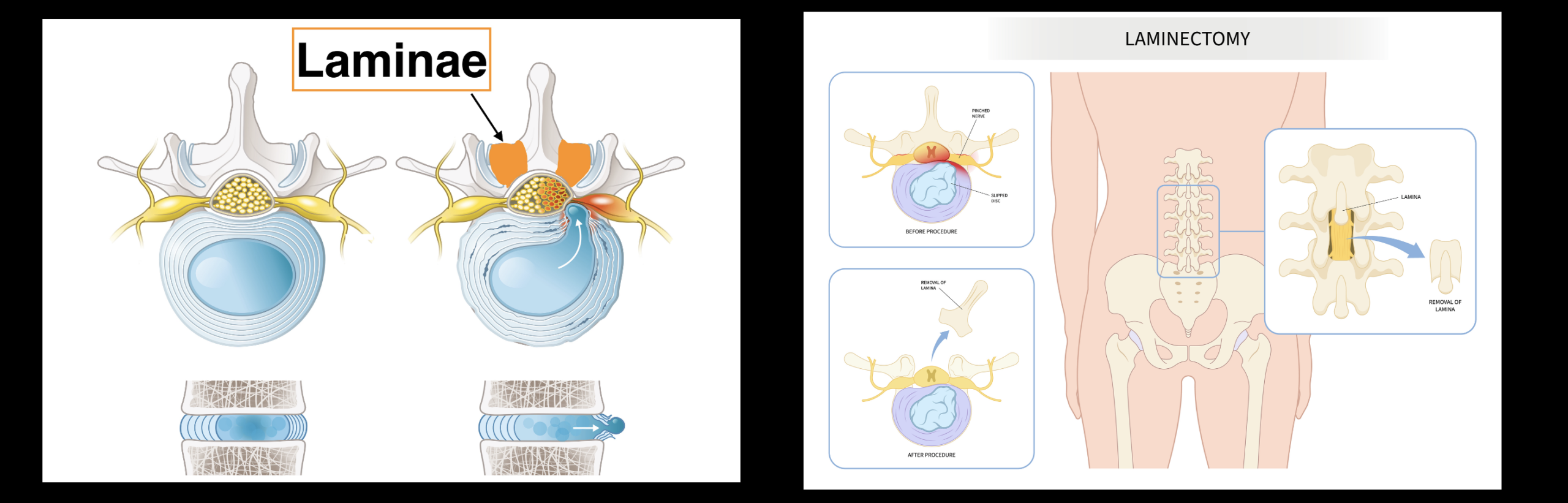
- Decompression Surgery: Laminectomy involves removal of part or all of the lamina to relieve pressure on neural structures. This may be performed using minimally invasive techniques to reduce recovery time and complications.
- Tumor Resection: Surgical removal of lesions involving posterior vertebral elements, often requiring a multidisciplinary approach.
- Spinal Fusion: Performed in cases of instability, commonly in conjunction with decompression.
Surgical intervention is generally reserved for cases involving progressive neurological deficits, structural instability, or pain refractory to comprehensive non-surgical care.
Outcomes and Prognosis
With accurate diagnosis and appropriate treatment, many patients experience meaningful pain reduction and functional improvement. Prognosis depends on underlying pathology, neurological involvement, and timely intervention.
Conclusion
Conditions affecting the lamina can result in significant pain and functional impairment. Accurate diagnosis and appropriate escalation of care are essential. When conservative measures are insufficient, interventional and surgical options provide effective symptom relief and improved quality of life.
Dr. Amit Sharma & our minimally invasive pain & spine team.
FAQ
What is the lamina in the spine?
The lamina is a part of each vertebra forming the posterior section of the vertebral arch. It helps form the vertebral canal that protects the spinal cord and nerve roots.
Can lamina problems cause back pain?
Yes. Conditions such as fractures, stenosis-related thickening, degenerative changes, or tumors can contribute to pain and may be associated with neurological symptoms.
How are lamina-related conditions diagnosed?
Diagnosis typically includes a clinical exam plus imaging such as X-rays, MRI, CT scans, and sometimes bone scintigraphy depending on suspected pathology.
What interventional treatments can help?
Depending on the cause, options may include image-guided corticosteroid injections, radiofrequency ablation, vertebroplasty or kyphoplasty in select fracture cases, and decompression surgery when significant compression is present.
When is laminectomy considered?
Laminectomy may be considered for severe stenosis or nerve compression, progressive neurological deficits, or refractory symptoms after non-surgical care. Fusion may be added if instability is present.
What symptoms require urgent evaluation?
Progressive weakness, bowel or bladder changes, saddle anesthesia, major trauma, fever/suspected infection, unexplained weight loss, or severe night pain—especially with neurological changes—require urgent medical evaluation.
References
- Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: ACP and APS clinical practice guideline. Ann Intern Med. 2007.
- Manchikanti L, Singh V, Falco FJ, et al. Epidural steroid injections for chronic spinal pain. Pain Physician. 2009.
- Friedly JL, Comstock BA, Turner JA, et al. Long-term effects of repeated injections for lumbar stenosis. Arch Phys Med Rehabil. 2017.
- Borenstein DG. Diagnostic evaluation and treatment of low back pain. Curr Opin Rheumatol. 2001.
- North American Spine Society. Evidence-Based Clinical Guidelines (Spine.org).



