
DRG Stimulation: 5 Critical Facts That Improve Pain
DRG Stimulation: 5 Critical Facts That Improve Pain
DRG Stimulation
Dorsal root ganglion (DRG) stimulation is a form of neuromodulation designed to help manage certain types of chronic, difficult-to-treat pain that stays localized, especially in the foot, ankle, knee, groin, or lower leg. Unlike long-term opioid therapy, DRG stimulation aims to reduce pain by delivering targeted electrical stimulation to a small bundle of sensory nerves called the dorsal root ganglion.
DRG stimulation is most commonly used for Complex Regional Pain Syndrome (CRPS) and related focal neuropathic pain patterns. If your pain is localized and persistent despite appropriate conservative treatments, DRG therapy may be an option to discuss with your pain specialist.
Learn more about CRPS from MedlinePlus and about pain terminology and definitions from the International Association for the Study of Pain (IASP). You can also compare DRG therapy with Spinal Cord Stimulation and review our office locations.
Indications
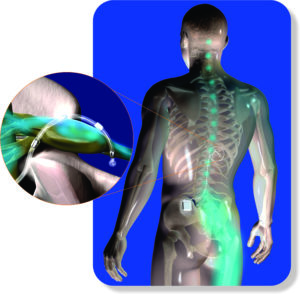
DRG stimulation involves placing a thin lead (wire) through the epidural space to target specific dorsal root ganglia. It is used as an aid in the management of moderate to severe, chronic, intractable pain of the lower limbs in adult patients with Complex Regional Pain Syndrome (CRPS) types I or II.
In the ACCURATE clinical study, participants had failed to achieve adequate pain relief despite trials of pharmacologic therapy across multiple drug classes and continued their medications during the study period. For readers who want to explore the published evidence, you can search peer-reviewed studies on PubMed.
Terminology note: In 1994, a consensus group convened by IASP reviewed diagnostic criteria and renamed reflex sympathetic dystrophy (RSD) and causalgia as complex regional pain syndrome (CRPS) types I and II, respectively.
How DRG Therapy Works
The dorsal root ganglion (DRG) is located near the spine and contains densely packed sensory nerve cell bodies. It acts like a “signal checkpoint” where sensory input, including pain, is organized before traveling to the spinal cord and brain. By stimulating the DRG, pain signals can often be reduced in a highly targeted region, which is why DRG therapy can be especially helpful when pain remains confined to a specific area.
Dorsal Root Ganglion (DRG)
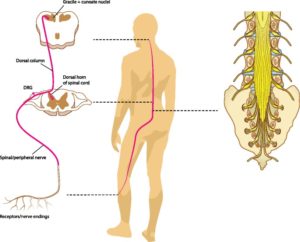
A dorsal root ganglion (also called a spinal ganglion or posterior root ganglion) is a cluster of nerve cell bodies located in the dorsal root of a spinal nerve. These sensory neurons carry information into the central nervous system. The DRG lies near the intervertebral foramen, where spinal nerve roots join.
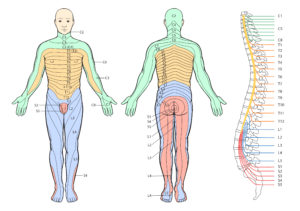
A dermatome is an area of skin supplied mainly by a single spinal nerve. There are 8 cervical nerves (C1 typically has no dermatome), 12 thoracic nerves, 5 lumbar nerves, and 5 sacral nerves. DRG stimulation is often considered when pain closely follows a dermatomal pattern and remains localized.
If your pain follows a dermatomal distribution and you have exhausted appropriate non-surgical options, it may be time to discuss DRG stimulation. Watch the video below to learn more about dermatomes and why they matter in targeted neuromodulation.
For a quick reference, see an overview of dermatomes at Physio-Pedia.
DRG stimulation is typically considered when pain is chronic, function-limiting, and localized, especially in the lower extremity or groin. It is most commonly used for CRPS, but may be discussed for other focal neuropathic pain patterns depending on your diagnosis and prior treatment response.
- Localized pain (for example: foot/ankle, knee, groin) that remains in a specific region
- CRPS type I or II (or a closely related pain pattern), as determined by your physician
- Inadequate relief from appropriate conservative options (medications, physical therapy, injections, and other treatments)
- Ability to participate in follow-up visits, device programming, and activity precautions during healing
Many practices use a short trial period to confirm that stimulation meaningfully improves pain and function before moving to permanent implantation. To discuss candidacy, you can request an appointment.
Procedure
Before the procedure
Your team will review your medications and medical history. If you take blood thinners or antiplatelet medication (for example, clopidogrel or warfarin), you may need a specific plan to hold or adjust them safely. Follow your physician’s instructions closely. You may also be asked not to eat or drink for several hours before the procedure.
During the procedure
- Patients are monitored closely and may receive sedation (often “monitored anesthesia care”), depending on the case and comfort needs.
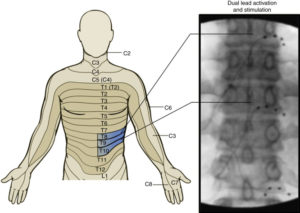
- Using live X-ray guidance (fluoroscopy), the physician advances a needle and places the lead(s) to target the appropriate DRG level(s).
- The goal is to achieve coverage of the painful area while maintaining safe lead placement.
Typical steps
- Positioning for comfort and safety
- Skin preparation and sterile technique
- Fluoroscopic imaging to identify the entry point and target
- Placement of a cannula (needle) under live imaging
- Placement of the DRG lead(s) through the needle
- Testing and programming to optimize coverage of the painful region
- Securing the lead(s); if permanent implant, connecting lead(s) to the generator
- Recovery monitoring and discharge instructions
After the procedure, you will receive activity restrictions, wound care guidance, and follow-up instructions. Programming adjustments are common in the early period and can significantly improve results.
Expected Results
DRG stimulation is designed to reduce pain and improve function, but results vary. Many patients aim for meaningful improvement such as better sleep, improved walking tolerance, and reduced flare intensity or frequency. A successful trial is typically used to help predict benefit before permanent implantation.
It is common to require several programming visits early on. Programming is essentially “tuning” the therapy so it matches your pain map as closely as possible.
Risks and Complications
All procedures have risks. Your physician will review these with you in detail based on your medical history. Potential risks include:
- Bleeding or bruising at the needle insertion site
- Infection
- Lead migration (movement) or device-related discomfort
- Inadequate pain coverage or loss of effectiveness over time
- Nerve irritation or injury (rare)
- Worsening pain or flare (sometimes temporary)
- Need for revision procedure or device replacement over time
Seek urgent medical attention for fever, severe increasing redness or swelling at the site, new progressive weakness, loss of bowel or bladder control, or severe unrelenting back or leg pain after a procedure.
Credits & Sources:
-
Van Buyten JP. Dorsal Root Ganglion Stimulation. Essentials of Pain Medicine, Page: 683-692. e1. Publication Year 2018.
-
Deer TR, Levy RM, Kramer J, et al. Dorsal root ganglion stimulation yielded higher treatment success rate for complex regional pain syndrome and causalgia at 3 and 12 months: a randomized comparative trial. Pain. 2017;158(4):669-681.
-
St. Jude Medical™ Proclaim™ DRG Neurostimulation System Clinician’s Manual. Plano, TX. 2017.
-
Graham RD, Sankarasubramanian V, Lempka SF. Dorsal Root Ganglion Stimulation for Chronic Pain: Hypothesized Mechanisms of Action. J Pain. 2022 Feb;23(2):196-211. doi: 10.1016/j.jpain.2021.07.008. Epub 2021 Aug 20. PMID: 34425252; PMCID: PMC8943693.
- https://www.physio-pedia.com/Dermatomes



