
Tarlov Cyst Solutions: 7 Proven Treatments You Should Know
Tarlov cysts (also called perineural cysts) are cerebrospinal fluid (CSF)-filled sacs that develop along spinal nerve roots, most often in the sacral spine. Many are found incidentally on MRI and never cause symptoms. When symptoms do occur, they can be life-disrupting and may mimic more common problems like disc disease or sciatica.
This page focuses on a practical question patients and clinicians both ask: Is the cyst truly the cause of my symptoms, and what are the best next steps? For related pain patterns, also review our pages on Low Back Pain and Pinched Nerve Root.
Basic Anatomy of Tarlov Cysts
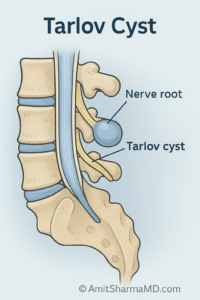
Tarlov cysts are usually located near the dorsal (sensory) nerve root sleeves, commonly around S2 and S3. They are dilations of the nerve root sheath filled with CSF. Some cysts can widen bony openings (foramina) or irritate adjacent nerve fibers, which is one reason symptoms can include both pain and sensory changes.
 |
 |
Epidemiology
Prevalence estimates vary widely depending on the population studied and whether imaging includes dedicated sacral sequences. Many studies report a range roughly from 1.5% to 13%, and cysts are reported more often in women than men. Importantly, not all cysts are symptomatic. A meaningful subset can cause symptoms, but a large portion remain incidental findings.
Clinical Presentation
When symptomatic, Tarlov cysts can cause symptoms that overlap with common spine diagnoses. Clues that raise suspicion include pain that is worse with sitting, worse with standing/walking in some cases, and symptoms that match sacral nerve distributions.
- Low Back Pain: Often chronic and may worsen with prolonged sitting or standing.
- Radicular Pain: Pain radiating into the buttock, leg, or foot depending on affected nerve roots.
- Sensory Disturbances: Numbness, tingling, burning, or “electric” sensations.
- Motor Symptoms: Weakness may occur in more severe cases.
- Pelvic/Sacral Symptoms: Perineal pain, genital sensory symptoms, or tailbone-area pain.
- Bowel/Bladder Changes: Urgency, retention, or dysfunction in selected cases.
Work-Up and Diagnosis
Diagnosis is not just “seeing a cyst on MRI.” The key is establishing whether the cyst matches the symptom pattern and whether other common causes explain symptoms better.
- Clinical Evaluation: Pain mapping, neurologic exam, gait assessment, and symptom triggers.
- MRI: Often the first-line study and the best overall tool to visualize cyst size, location, and nerve root relationship.
- CT Myelography: Helps evaluate communication with the CSF space and can be used in selected cases for procedural planning.
- Electrodiagnostic Testing (EMG/NCS): May help differentiate peripheral neuropathy vs. radiculopathy and assess nerve function in selected cases.
Incidental vs. Clinically Significant
Many Tarlov cysts are incidental. A cyst is more likely to be clinically significant when: (1) symptoms correlate with sacral nerve distributions, (2) pain is persistent and function-limiting, (3) imaging shows features suggesting nerve irritation/compression, and (4) targeted diagnostic procedures produce meaningful symptom change.
Tarlov Cyst Solutions: 7 Evidence-Informed Treatments
There is no one-size-fits-all treatment. The best plan depends on symptom severity, neurologic findings, imaging, and whether the cyst is truly the pain generator. Below are the most common options discussed in clinical practice, starting with the least invasive.
-
Observation and Education (Most Common)
If the cyst is incidental and symptoms do not correlate, the safest approach is often observation. This includes monitoring symptoms, addressing other spine diagnoses, and avoiding procedures that add risk without clear benefit.
-
Conservative Symptom Management
For mild to moderate symptoms, conservative strategies may include activity modification, targeted physical therapy, non-opioid medications, and treatment of overlapping conditions (disc disease, stenosis, SI joint pain, pelvic floor dysfunction). The goal is improved function while minimizing medication burden.
-
Image-Guided Injections (Selected Cases)
Some patients benefit from targeted injections when there is overlap with inflammatory radicular pain or adjacent pain generators. These injections are not “cyst treatments,” but can help clarify what is driving symptoms and provide symptom control in appropriate cases.
-
CT-Guided Aspiration (Often Diagnostic, Often Temporary)
CT-guided aspiration can sometimes provide temporary relief and may help confirm that the cyst is symptom-relevant. However, aspiration alone often has a higher chance of re-accumulation, which is why aspiration is frequently paired with sealing techniques when appropriate.
-
Percutaneous Aspiration with Fibrin Sealant (Minimally Invasive Option)
In carefully selected symptomatic patients, aspiration followed by fibrin sealant injection is a minimally invasive approach intended to reduce refilling and improve symptoms. Outcomes vary, and recurrence can still occur, but this is often considered before open surgery for eligible patients.
-
Microsurgical Techniques (Fenestration/Imbrication/Wrapping)
Surgery may be considered when symptoms are clearly attributable to the cyst and conservative or minimally invasive options have failed. Microsurgical strategies aim to decompress the cyst, reduce CSF pressure effects, and protect the nerve root. Surgical decision-making is highly individualized because benefits must be weighed against complication risk.
-
Multimodal Pain Management and Neuromodulation (Selected Cases)
For refractory chronic pain or when mechanical decompression is not appropriate, a comprehensive pain plan may include medications, functional restoration, behavioral pain strategies, and in select cases neuromodulation. The target here is function and quality of life, especially when structural “fixes” are unlikely to fully resolve symptoms.
Conclusion
Tarlov cysts are common enough to be seen on many MRIs, but symptomatic Tarlov cysts are a different category and require careful correlation with symptoms and exam findings. If your symptoms fit a sacral nerve distribution and have not improved with appropriate conservative care, a specialist evaluation can help determine whether the cyst is incidental or clinically meaningful and which treatment path is most reasonable.
For patients on Long Island seeking evaluation and evidence-informed treatment options, visit our Services page or contact us to request a consultation. You can also find us at Office Locations.
Frequently Asked Questions (FAQ)
Are Tarlov cysts dangerous?
Most Tarlov cysts are harmless and asymptomatic. However, a subset can compress or irritate nerve roots and cause pain or neurologic symptoms that warrant targeted evaluation.
When should a Tarlov cyst be treated?
Treatment is considered when symptoms correlate with cyst location and are persistent or progressive despite conservative care, particularly if there are neurologic deficits or significant bladder/bowel symptoms.
Is surgery the only option for Tarlov cysts?
No. Minimally invasive options such as CT-guided aspiration with fibrin sealant may be considered for selected patients before surgery. Many cysts require no intervention at all.
Can Tarlov cysts recur after treatment?
Yes. Recurrence or symptom persistence is possible, especially after aspiration alone. Procedures designed to reduce refilling aim to lower recurrence risk, but outcomes vary.
Dr. Amit Sharma & our minimally invasive pain & spine team.



