
Coccyx Tailbone Injection
Coccyx Tailbone Injection is a targeted, minimally invasive treatment designed to relieve persistent pain in the lower spine. Often caused by trauma, prolonged sitting, or childbirth, tailbone pain—also known as coccydynia—can be debilitating and resistant to traditional therapies. Coccyx tailbone injection delivers anti-inflammatory medication directly to the affected area, offering fast and localized relief while also serving as a diagnostic tool. For patients seeking a non-surgical option to manage coccyx pain, this procedure is safe, effective, and performed under image guidance for maximum precision.
Coccyx
The coccyx is the terminal segment of the spine that consists of 3 to 5 fused bone segments. It attaches to sacrum with sacrococcygeal ligament. Coccyx has several important functions. It acts as the insertion site for multiple muscles, ligaments, and tendons, which help support the pelvic floor and also contribute voluntary bowel control. Coccyx also serves as one leg of the tripod, and along with the ischial tuberosities, provides weight-bearing support to a person in the seated position. Coccyx also provides positional support to the anus.
Coccygeal Plexus
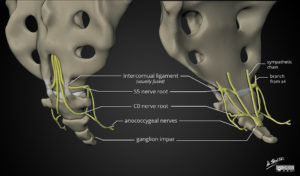
Coccyx receives nerve supply from a network of nerves, the coccygeal plexus (Courtesy of Dr Matt Skalski, Radiopaedia.org. From the case rID: 63690). Blocking coccygeal nerves or coccygeal plexus has been shown to help with coccydynia or tailbone pain.
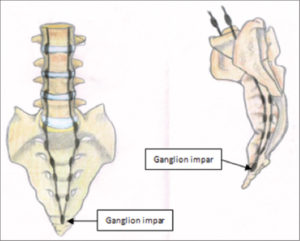
Ganglion of Impar (Courtesy: Asian Journal of Neurosurgery)
In addition, the pelvic portion of each sympathetic trunks converge and end on the front of the coccyx in a small ganglion, the ganglion impar, also known as azygos or ganglion of Walther. There is a strong evidence that this bundle of nerves also carries pain signals in cases of coccydynia. Blocking coccygeal nerves (or coccygeal plexus) along with the ganglion of impar, has been shown to help with coccydynia or tailbone pain. Imaging guidance, such as fluoroscopy, is absolutely recommended for injections around the coccyx because of its position relative to other vital structures.
Coccydynia
Coccydynia, or coccygodynia, is pain in the region of the coccyx or tailbone. Treatment of tailbone or coccygeal pain can be difficult and sometimes controversial because of the multifactorial nature of coccygeal pain. Many physiologic and psychological factors contribute to its cause. Most cases of coccydynia resolve within weeks to months with or without conservative treatment, but for a few patients, the pain can become chronic and debilitating.
Obesity and female gender are often cited as predisposing factors to develop tailbone pain. Women are 5 times more likely to develop coccydynia than men. Presumably, rapid weight loss can also be a risk factor because of the loss of mechanical cushioning. The most common cause of coccydynia is external or internal trauma. External trauma usually occurs due to a backwards fall, leading to a bruised, dislocated, or broken coccyx. The location of the coccyx makes it particularly susceptible to internal injury during childbirth, especially during a difficult or instrumented delivery. Minor trauma can also occur from repetitive or prolonged sitting on hard, narrow, or uncomfortable surfaces. Nontraumatic coccydynia can result from hypermobility or hypomobility of the sacrococcygeal joint.
Conservative treatment is successful in 90% of coccydynia cases. Relatively simple measures like a modified wedge-shaped cushions (coccygeal cushions) or circular cushions (donut cushions) have been suggested for the treatment of coccydynia. Coccygeal cushions can relieve the pressure on the coccyx while the patient is seated. Donut cushions can place pressure on the coccyx by isolating the coccyx and ischial tuberosities and are more useful for treating rectal pain. Postural training, heat and cold applications and antiinflammatory medications are helpful in many cases.

For the few cases that do not respond to these conservative treatments, more aggressive treatments may be indicated. Pelvic floor rehabilitation can be helpful for coccydynia that is associated with pelvic floor muscle spasms. Manual manipulation and massage can be both diagnostic and therapeutic. Intrarectal manipulation can identify and potentially correct a dislocated sacrococcygeal joint. Manual manipulation and massage can help relieve associated muscle spasms or ligament pain.
In a handful of cases, a combination of coccygeal nerve block and ganglion of impar block with a distal caudal epidural injection (coccyx tailbone injection) has been shown to an extremely successful treatment option to resolve pain. Surgical resection of coccyx (coccygectomy) is rarely needed.
Coccyx Tailbone Injection
Ganglion of Impar Injection (Courtesy: Ainsworth Institute)
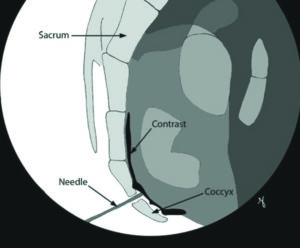
You may be given a laxative the night before coccyx tailbone injection to keep your rectum “empty”. After admission process is completed, you will be taken to the procedure suite. You will be positioned in a comfortable position and anesthesia is induced by an attending anesthesiologist. Fluoroscopic images (X-Ray) is used to identify the site of needle entry. A thin Cannula (needle) is placed under live fluoroscopic guidance to the target sacrococcygeal opening and various safety steps are conducted to confirm accurate location. Injection of planned medication is made and needle are withdrawn out of sacrococcygeal space.
Needle is then redirected to block sacrococcgeal nerves. Needle is finally withdrawn. A band-aid is applied at the needle entry site and patient is taken to recovery area. In certain cases, a small dose is also injected in the distal epidural space at S2-4 level as part of the coccyx tailbone injection.
In selective cases, regenerative medicine options like platelet rich plasma treatment may be offered as an alternative to steroids for coccyx tailbone injection. Platelet-rich-plasma (PRP) injections use components of the body’s own blood to stimulate healing. Platelets, which are usually associated with coagulation (clotting), may assist in mending and strengthening damaged tissue by increasing certain growth factors.
During the normal healing process, the body uses platelets to promote new-tissue growth and repair injuries. By supplementing platelet content, the healing process is accelerated. There is ongoing research on the efficacy of PRP injections, and some medical professionals remain skeptical about their value.
Last, but not the least, if you do not benefit from coccyx tailbone injection, DRG stimulation has shown some positive results in treatment of coccydynia and it might be worth a trial before you ever consider coccygectomy.
What is Coccydynia?
Coccydynia, or coccyx pain, is often multifactorial and may result from trauma, prolonged sitting, or childbirth. Most cases resolve with conservative care such as cushions, posture correction, and anti-inflammatories.
Benefits of Coccyx Tailbone Injection
- Provides rapid and localized pain relief
- Reduces inflammation and nerve sensitivity
- Used as a diagnostic tool to confirm pain source
- Can delay or avoid need for surgical intervention
- Minimally invasive with quick recovery
Regenerative Medicine Options
Regenerative medicine can complement or replace steroid-based Coccyx Tailbone Injections. Platelet-rich plasma (PRP) uses platelets to boost healing in damaged tissue. This is especially useful in chronic tailbone pain unresponsive to traditional therapies.
Emerging technologies like DRG stimulation are being studied for cases of coccydynia that are resistant to conservative or interventional management.
Risks and Complications
- Bleeding or bruising at the needle site
- Infection
- Nerve injury
- Temporary aggravation of symptoms
Summary
Coccyx Tailbone Injection is a proven interventional treatment for chronic tailbone pain, offering targeted relief through precise, image-guided delivery of anti-inflammatory medication. It’s especially effective for patients with coccydynia that hasn’t responded to conservative care. When paired with options like platelet-rich plasma (PRP) or pelvic floor therapy, this injection can significantly improve quality of life without surgery. Safe, fast, and minimally invasive, it remains a cornerstone in modern spine and pain management.
Frequently Asked Questions About Coccyx (Tailbone) Injections
What is a coccyx injection?
A coccyx injection involves administering a combination of a local anesthetic and corticosteroid directly into the area surrounding the tailbone (coccyx). This procedure aims to reduce inflammation and alleviate pain associated with conditions like coccydynia. It is typically performed under imaging guidance, such as fluoroscopy or ultrasound, to ensure precise needle placement.
Who is a candidate for this procedure?
Individuals experiencing chronic tailbone pain that has not responded to conservative treatments—such as physical therapy, oral medications, or lifestyle modifications—may be considered candidates for a coccyx injection. A thorough evaluation by a healthcare provider is necessary to determine suitability for the procedure.
What can I expect during the procedure?
The procedure is usually conducted on an outpatient basis. After positioning you appropriately, the healthcare provider will cleanse the injection site and administer a local anesthetic to numb the area. Using imaging guidance, a needle is then inserted to deliver the anesthetic and steroid mixture to the targeted region. The entire process typically takes about 15 to 30 minutes.
How soon will I experience relief, and how long will it last?
Some patients may experience immediate pain relief due to the local anesthetic, while the corticosteroid’s anti-inflammatory effects generally take a few days to manifest. The duration of pain relief varies among individuals, ranging from several weeks to several months. Repeat injections may be considered based on the patient’s response and clinical guidelines.
Are there any risks or side effects?
While coccyx injections are generally safe, potential risks include infection, bleeding, allergic reactions, and temporary increases in pain. Some patients may experience side effects related to corticosteroids, such as elevated blood sugar levels or menstrual irregularities. It’s essential to discuss any concerns with your healthcare provider before the procedure.
What should I do after the injection?
Post-procedure, patients are usually advised to rest for a short period and avoid strenuous activities for at least 24 hours. Applying ice to the injection site can help reduce discomfort. It’s important to follow your healthcare provider’s specific aftercare instructions to ensure optimal recovery.
Can I drive myself home after the procedure?
Due to the effects of the local anesthetic and potential discomfort following the injection, it’s recommended to arrange for someone to drive you home after the procedure.
How many injections can I receive?
The number of coccyx injections a patient can receive varies based on individual response and clinical guidelines. Typically, healthcare providers limit the number of steroid injections to minimize potential side effects. It’s crucial to have a personalized treatment plan discussed with your provider.
What if the injection doesn’t relieve my pain?
If the coccyx injection does not provide sufficient pain relief, alternative treatments may be considered. These can include physical therapy, nerve blocks like the ganglion impar block, or, in rare cases, surgical options such as coccygectomy. Your healthcare provider will guide you through the available options based on your specific condition.
References
- Lirette LS et al. Coccydynia Overview. Ochsner J. 2014
- StatPearls: Coccygeal Anatomy
- Toshniwal GR et al. Ganglion impar block study. Pain Physician. 2007
- Buttaci CJ, Foye PM, Stitik TP: Coccydynia successfully treated with ganglion impar blocks: A case series. Am J Phys Med Rehabil 2005;84:218.
- Lirette LS, Chaiban G, Tolba R, Eissa H. Coccydynia: an overview of the anatomy, etiology, and treatment of coccyx pain. Ochsner J. 2014;14(1):84-87.
- Foye PM, Buttaci CJ, Stitik TP, Yonclas PP. Successful injection for coccyx pain. Am J Phys Med Rehabil. 2006 Sep;85(9):783–784.
- Plancarte R, Amescua C, Patt RB, Allende S. Presacral blockade of the Ganglion of Walther (Ganglion Impar) Anesthesiol. 1990 Sep;73(3A):A751.
- Toshniwal GR, Dureja GP, Prashanth SM. Transsacrococcygeal approach to ganglion impar block for management of chronic perineal pain: a prospective observational study. Pain Physician. 2007 Sep;10(5):661–666.
- Mostafa E, Varacallo M. Anatomy, Back, Coccygeal Vertebrae. [Updated 2020 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549870/



