L5 Pain: 5 Important Insights for Relief
If you have sharp or aching pain running from your lower back into your hip, outer thigh, or down toward the top of your foot and big toe, there is a good chance the L5 nerve root is involved. L5 Pain can feel confusing—sometimes it starts in the back, sometimes mostly in the leg—and many patients are told different names such as “sciatica,” “pinched nerve,” or “radiculopathy.” Understanding what L5 Pain really means is the first step toward the right treatment plan.
Quick Summary:L5 Pain usually refers to irritation or compression of the L5 nerve root in the lower spine. This can cause low back or buttock pain with radiation down the outer thigh, outer calf, and onto the top of the foot and big toe, sometimes with numbness or weakness when lifting the foot. The most common causes are disc herniation, foraminal stenosis, and age-related spine changes. A focused exam, imaging when needed, and minimally invasive treatments can often calm L5 Pain without surgery.
Understanding L5 Radicular Pain and the L5 Nerve Root
The spinal cord ends around the L1–L2 level as the conus medullaris. Below this point, the nerves no longer travel inside a solid cord—instead, they continue downward as individual nerve fibers called the cauda equina (“horse’s tail”). Each lumbar nerve root descends several levels inside the spinal canal before exiting through its specific foramen.
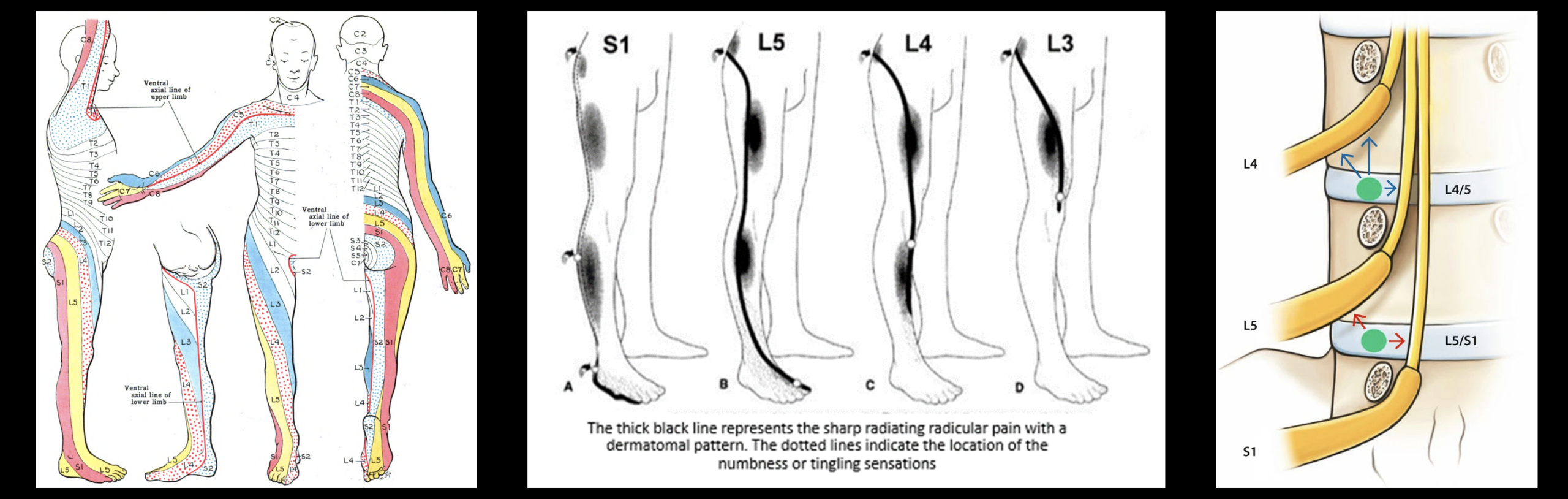
The L5 nerve root originates at the L5 segment of the spinal cord but then travels downward inside the canal as a traversing root. It passes behind the L4–L5 disc and continues caudally until it exits the spine through the L5–S1 neural foramen as an exiting root.
This anatomy explains why L5 Pain can come from two different locations:
- L4–L5 level: A disc herniation or stenosis here can compress the traversing L5 root inside the canal.
- L5–S1 level: Foraminal or far-lateral narrowing can compress the exiting L5 root as it leaves the spine.
Once outside the spine, the L5 nerve contributes to the lumbosacral plexus and supplies sensation to the outer leg, top of the foot, and big toe, as well as motor control to muscles that lift the foot and extend the big toe. Irritation anywhere along this path can produce the classic pattern of L5 Pain.
In many patients, L5 Pain shows up as:
- Pain in the lower back or lumbosacral area that may radiate into the buttock.
- Shooting or burning pain down the outer thigh and outer calf.
- Symptoms on the top of the foot and into the big toe (L5 dermatome).
- Possible weakness when lifting the foot or big toe (trouble with heel-walking).
- Numbness, tingling, or “pins and needles” in the same pattern.
Because L5 sits in the lower spine, L5 Pain often overlaps with what many people call “sciatica.” In medical terms, this is a form of lumbar radiculopathy involving the L5 nerve root.
Common Causes of L5 Radicular Pain
L5 Pain can occur when the L5 nerve root is irritated anywhere along its course—either while it is traversing the spinal canal at the L4–L5 level or while it is exiting the spine through the L5–S1 foramen. This distinction matters, because different spine levels can affect the same L5 nerve root in different ways.
Common structural causes include:
- L4–L5 disc herniation (traversing L5 root): At this level, the disc typically compresses the L5 nerve root before it exits the spine. This is the most frequent cause of true L5 radiculopathy.
- L5–S1 foraminal or far-lateral stenosis (exiting L5 root): Narrowing where the L5 nerve root actually exits the spine can pinch or inflame the root, especially with disc height loss or facet hypertrophy.
- Degenerative disc disease: Loss of disc height at either level (L4–L5 or L5–S1) can cause the foramen to collapse and compress the L5 nerve root.
- Spondylolisthesis: Forward slippage of L4 on L5 or L5 on S1 can stretch or compress the traveling or exiting L5 root.
- Facet joint arthropathy: Arthritic enlargement of the facet joints can narrow the space around the L5 root, contributing to L5 Pain.
- Epidural cysts, synovial cysts, tumors, infections, or trauma: Less common but important structural causes that may compress the L5 nerve root at any point along its path.
In an accurate evaluation of L5 Pain, your specialist will determine whether the L5 nerve is being affected at the L4–L5 level (traversing root) or at the L5–S1 level (exiting root), since the imaging findings and treatment strategy can differ significantly.
5 Essential Relief Insights for L5 Pain
Every case of L5 Pain is unique, but several core principles can guide a safer and more effective path to relief.
Insight 1: Recognize Classic L5 Pain Patterns
- Pain or burning in the lower back or buttock with radiation down the outer thigh and outer calf.
- Tingling or numbness on the top of the foot and into the big toe.
- Weakness when trying to lift the big toe or foot toward the shin (difficulty walking on heels).
- Pain worsened by sitting, bending forward, lifting, or twisting.
When patients describe this combination, L5 Pain becomes a primary consideration rather than more general back or leg pain.
Insight 2: Differentiate L5 Pain from Other Levels and Conditions
L5 Pain is only one piece of the radiculopathy picture. For example:
- L4 involvement may cause pain and numbness more in the front of the thigh and knee, with weaker knee extension.
- S1 involvement may cause pain down the back of the calf and into the sole of the foot, with difficulty walking on tiptoes.
- Hip arthritis, peripheral neuropathy, and vascular issues can also mimic some leg symptoms.
Sorting out L5 Pain from these other patterns is essential. This is why your provider will ask detailed questions and perform a focused neurologic exam rather than relying on imaging alone.
Insight 3: The Role of Exam and Imaging in L5 Pain
A focused exam is the most important first step in diagnosing L5 Pain. Because the L5 nerve root controls specific muscles and sensory regions, your specialist may uncover:
- Weakness in ankle dorsiflexion (lifting the foot) or big toe extension (extensor hallucis longus weakness).
- Sensory changes over the outer calf, top of the foot, and big toe.
- Positive straight-leg raise if nerve tension provokes the same radiating symptoms.
- Difficulty heel-walking due to L5 motor involvement.
Imaging is then used to determine exactly where the L5 root is irritated:
- MRI at L4–L5: Looks for compression of the traversing L5 root by disc herniation, stenosis, or ligament hypertrophy.
- MRI at L5–S1: Looks for compression of the exiting L5 root by foraminal narrowing, disc collapse, bone spurs, or far-lateral disc herniations.
This “two-level check” is critical. Many patients with L5 Pain have a normal L5–S1 disc but a large L4–L5 disc herniation affecting the traversing L5 root. Others have a relatively normal L4–L5 disc but a collapsed L5–S1 foramen pinching the exiting root. Matching exam findings with imaging is what leads to the correct diagnosis.
Insight 4: Non-Surgical Relief Strategies for L5 Pain
Many patients with L5 Pain improve without surgery, especially when treatment is started early and tailored properly.
Common non-surgical strategies include:
- Activity modification: Short periods of relative rest, then gradual return to movement while avoiding heavy lifting and twisting.
- Medications: Anti-inflammatory medications, short courses of oral steroids when appropriate, neuropathic pain agents, and muscle relaxants.
- Physical therapy: Core and hip strengthening, posture training, nerve mobilization, and education about spine mechanics.
- Ergonomic changes: Adjusting sitting posture, workstation setup, and how you bend, lift, and carry during the day.
In some cases of persistent L5 Pain, interventional options can be considered:
- Epidural steroid injections: To reduce inflammation around the L5 nerve root.
- Selective L5 nerve root blocks: To confirm the pain generator and provide targeted relief.
- Other minimally invasive procedures tailored to the underlying cause.
These approaches often work alongside a structured rehab program rather than replacing it.
Insight 5: When L5 Pain Warrants a Higher Level of Intervention
In L5 radiculopathy, decisions about injections or surgery depend heavily on which portion of the nerve root is compressed and how severe the findings are.
- Traversing L5 root compression (L4–L5): Large central or paracentral disc herniations may respond to epidural injections but sometimes require microdiscectomy if weakness progresses.
- Exiting L5 root compression (L5–S1): Severe foraminal stenosis or far-lateral herniations may require a transforaminal epidural injection or foraminotomy to decompress the nerve.
- Progressive weakness: New difficulty lifting the foot or big toe is a sign of worsening L5 motor involvement and should prompt urgent evaluation.
- Cauda equina features: Although not specific to L5, bowel/bladder changes or saddle numbness indicate a surgical emergency.
Understanding whether the traversing or exiting L5 root is involved helps tailor the safest and most effective procedure, when needed.
Home Care and Self-Management Tips for L5 Pain
While you are being evaluated and treated, certain habits can help keep L5 Pain from spiraling out of control:
- Avoid prolonged slumped sitting; use a chair with good lumbar support.
- Change positions regularly—alternate sitting, standing, and short walks.
- Use proper body mechanics when lifting (bend at the hips and knees, keep objects close to your body).
- Maintain a healthy weight and stay as active as your pain allows.
- Follow any home exercise program recommended by your therapist or specialist.
These steps will not cure every case of L5 Pain, but they help reduce mechanical stress on the L5 region and support the rest of your treatment plan.
When to Seek Urgent Care for L5 Pain
Most cases of L5 Pain are painful but not dangerous. However, you should seek urgent or emergency medical attention if you experience:
- Sudden loss of bowel or bladder control.
- Severe numbness in the groin or saddle region.
- Rapidly worsening leg weakness or new foot drop.
- Fever, chills, or unexplained weight loss with back and leg pain.
- Back or leg pain after significant trauma, such as a fall or car accident.
These red-flag signs are not typical of straightforward L5 Pain and may signal something more serious that requires immediate evaluation.
Next Steps: Building a Plan for Your L5 Pain
Living with unresolved L5 Pain can affect everything from work and sleep to walking and exercise. The goal of a thoughtful, stepwise approach is to pinpoint how much of your pain is truly coming from the L5 nerve root, what structural issues are driving it, and which minimally invasive options are most likely to help.
If your symptoms line up with the patterns described here—or if you have been told you have an L4–L5 disc herniation, foraminal stenosis, or “L5 radiculopathy” but are unsure what to do next—consider consulting a specialist who regularly treats complex L5 Pain and related conditions such as chronic back pain and sciatica. A customized plan can help you move from uncertainty and flare-ups toward safer, longer-lasting relief.
Ready to Get Answers About Your L5 Pain?
If you have ongoing leg or foot symptoms and suspect L5 nerve involvement, a focused evaluation can help clarify the exact source of your L5 Pain and outline the safest, most effective treatment options—ranging from targeted therapy to image-guided injections and other minimally invasive approaches.
Schedule a consultation to review your MRI, exam findings, and prior treatments so we can build a personalized plan that addresses the true cause of your L5 Pain, not just the symptoms.
References
Theodoridis, T. (2023). Landmark-Assisted Infiltrations and Injection Techniques on the Cervical, Thoracic and Lumbar Spine. In: Jerosch, J. (eds) Minimally Invasive Spine Intervention. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-63814-9_4.



