
Cluneal Neuropathy: 7 Proven Ways to Relieve Pain Fast
Cluneal neuropathy is an often-overlooked cause of low back pain, buttock pain, and even pain that feels like sciatica. Many patients are told they have a disc problem, sacroiliac dysfunction, or nonspecific back pain, yet the real source may be irritation or entrapment of a small sensory nerve near the iliac crest. Because these nerves are tiny and easy to miss on standard imaging, cluneal neuropathy can hide in plain sight.
If you have persistent pain near the upper buttock, pain triggered by standing or walking, or tenderness along the back of the pelvis, this diagnosis deserves attention. In the right patient, identifying cluneal neuropathy can completely change the treatment path.
What Is Cluneal Neuropathy?
Cluneal neuropathy refers to pain caused by irritation, entrapment, or compression of the cluneal nerves. These are purely sensory nerves that supply the skin over the lower back, upper buttock, and nearby tissues. They do not control muscle strength, but when they become irritated, they can generate surprisingly intense pain.
The cluneal nerves are typically grouped into three categories:
- Superior cluneal nerves, which arise from lower thoracic and lumbar dorsal rami
- Middle cluneal nerves, which arise from sacral dorsal rami
- Inferior cluneal nerves, which are less commonly discussed in typical low back pain evaluations
Among these, the superior cluneal nerve entrapment pattern is the most widely recognized, but middle cluneal nerve irritation may also contribute to chronic pain syndromes.
Cluneal Neuropathy Anatomy
To understand why this condition is so tricky, it helps to understand the anatomy. The superior cluneal nerves travel from the lower back toward the buttock and cross over the iliac crest. At this point, some branches pass through tight fibro-osseous tunnels created by fascia and bone. That narrow passage can become the pain generator.
The middle cluneal nerves travel in the region of the sacroiliac area and may be compressed as they pass near or under the long posterior sacroiliac ligament. This is one reason symptoms may overlap with what many people assume is sacroiliac joint pain.
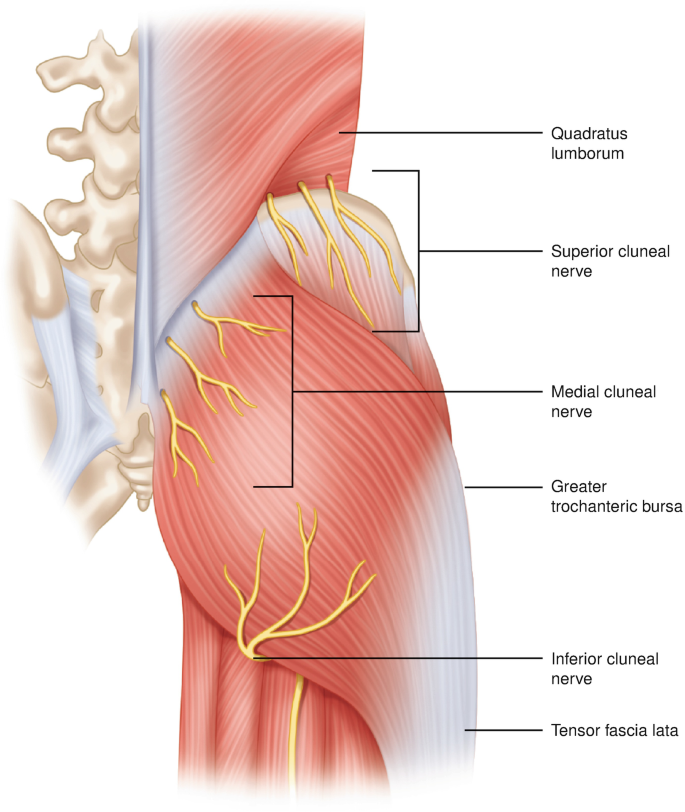
Illustration of cluneal nerve anatomy and the typical region where superior cluneal neuropathy can occur.
That anatomy matters. When these nerves are compressed at predictable points near the posterior iliac crest, patients may develop pain with standing, walking, bending, rolling in bed, or sitting for long periods. This pattern helps explain why cluneal neuropathy can mimic other spine disorders.
Why Cluneal Neuropathy Is Often Missed
Cluneal neuropathy is a master of disguise. It can imitate:
- Lumbar radiculopathy
- Sacroiliac region pain
- Facet-mediated pain
- Myofascial pain
- Persistent pain after spine surgery
Because the nerves are small, standard MRI and CT scans usually do not directly show the problem. That means a patient may have normal imaging, mildly abnormal imaging, or unrelated degenerative findings, while the real pain generator is a small entrapped sensory nerve.
That is exactly why this diagnosis belongs in the broader conversation about conditions mimicking spine diseases. A pain pattern that looks spinal is not always coming from the spine itself.
Symptoms of Cluneal Neuropathy
Cluneal neuropathy can cause a wide range of symptoms, but the classic presentation includes low back pain centered near the iliac crest or upper buttock. In some patients, the pain remains local. In others, it radiates in a way that mimics sciatica.
Common Symptoms
- Low back pain near the top of the buttock
- Focal tenderness along the posterior iliac crest
- Buttock pain
- Burning, aching, or sharp pain
- Pain worsened by standing, walking, bending, twisting, or sitting
- Pain that radiates into the buttock, hip, groin, or leg
- Pain when rolling over in bed
In many patients, cluneal neuropathy creates leg symptoms that can easily be mistaken for lumbar nerve root pain, which is one reason the diagnosis is so often delayed.
What Causes Cluneal Neuropathy?
The underlying issue is usually mechanical irritation or entrapment. These nerves pass through tight anatomical corridors, and repeated tension or compression may trigger symptoms.
Potential Causes and Contributors
- Repetitive bending and twisting
- Athletic overuse
- Paraspinal muscle tightness
- Abnormal posture or altered gait
- Degenerative spinal changes that alter body mechanics
- Prior lumbar surgery
- Vertebral compression fractures
- Increased muscle tone or movement disorders
Cluneal nerve irritation may be seen in patients whose posture, muscle tone, or spinal mechanics place repeated stress on these nerve pathways.
Cluneal Neuropathy vs Sciatica
This is where many patients get caught in the weeds. Sciatica usually refers to pain caused by irritation of a spinal nerve root, often from a disc herniation or spinal stenosis. Cluneal neuropathy, by contrast, is a peripheral nerve entrapment issue. The pain may feel similar, but the source is different.
That difference matters because treatment should target the correct structure. A person with cluneal neuropathy may not improve with treatments aimed only at a disc or spinal canal problem.
If you want a more focused discussion of one of the most common variants, see superior cluneal neuropathy.
How Cluneal Neuropathy Is Diagnosed
The diagnosis of cluneal neuropathy is largely clinical. In other words, it depends on the story, the exam, and the response to targeted treatment.
Important Diagnostic Clues
- Low back or buttock pain in the expected cluneal nerve distribution
- Symptoms worsened by posture or lumbar movement
- A trigger point over the posterior iliac crest or nearby sacroiliac region
- Reproduction of symptoms when that trigger point is pressed
- Temporary relief with a diagnostic nerve block
This is a big reason the physical examination matters. A careful clinician may identify a small, reproducible pain point that explains months or years of symptoms.
Can MRI or CT Diagnose Cluneal Neuropathy?
Usually not directly. Standard imaging often fails to visualize the tiny cluneal nerves themselves. Imaging is still useful because it helps rule out other causes or identify other issues that may coexist, but it does not reliably confirm cluneal neuropathy.
That is one reason so many patients are told their pain is nonspecific even when it is not. The structure causing the pain may simply be too small to show clearly on routine imaging.
Treatment Options for Cluneal Neuropathy
Treatment depends on the severity of symptoms, duration, prior care, and the certainty of diagnosis. In the right setting, treatment can be very effective.
1. Activity Modification and Conservative Care
Initial treatment may include avoiding aggravating movements, improving posture, reducing repetitive strain, and addressing surrounding muscle tension. Physical therapy may help some patients, especially if mechanics are contributing to nerve irritation.
2. Medications
Anti-inflammatory medication or neuropathic pain medication may provide partial relief, although medication alone often does not solve a true entrapment problem.
3. Diagnostic and Therapeutic Cluneal Nerve Blocks
Cluneal nerve blocks play a critical dual role in both diagnosing and treating cluneal neuropathy. Because these small sensory nerves are not typically visualized on standard imaging, targeted injections often provide the most reliable confirmation of the pain source.
During the procedure, a small amount of local anesthetic—sometimes combined with a corticosteroid—is placed around the suspected cluneal nerve. This allows the clinician to directly assess whether the nerve is responsible for the patient’s symptoms.
Why Cluneal Nerve Blocks Are So Important
- Diagnostic clarity: If the patient’s usual pain improves significantly after the injection, it strongly supports cluneal nerve involvement.
- Real-time feedback: The response to the block helps distinguish cluneal neuropathy from other causes of buttock pain such as sacroiliac joint dysfunction, piriformis syndrome, or lumbar radiculopathy.
- Guides further treatment: A positive response allows treatment to be focused on the cluneal nerves rather than pursuing unrelated spinal or joint interventions.
Therapeutic Benefit
In addition to confirming the diagnosis, cluneal nerve blocks may provide meaningful pain relief. Some patients experience substantial and lasting improvement after a single injection, particularly when the nerve irritation is mild or recent. In other cases, the relief may be temporary but still highly valuable in guiding the next step in treatment.
When the response is favorable but not sustained, additional treatment options—such as repeat blocks or other nerve-targeted therapies—may be considered based on the individual clinical scenario.
For a detailed overview of how the procedure is performed and what to expect, see our dedicated page on cluneal nerve block.
In practical terms, cluneal nerve blocks are often the turning point in patients with persistent buttock pain who have not responded to prior treatments. They help move the diagnosis from uncertainty to precision, which is essential for achieving lasting relief.
4. Minimally Invasive Procedures
Depending on the clinical setting, other image-guided or nerve-focused interventions may be considered when pain persists after simple conservative treatment.
5. Surgical Decompression or Neurolysis
When cluneal neuropathy is clearly identified and conservative care fails, surgical decompression may be appropriate. Published reports describe favorable outcomes after decompression of the entrapped nerve branches, including improvement in pain and function.
How to Choose the Right Treatment
The most effective treatment for superior cluneal neuropathy depends on both the severity of symptoms and the patient’s response to earlier therapies. In general, care follows a stepwise approach, but individual factors often guide the decision-making process.
- Mild or early symptoms: Conservative treatments such as physical therapy, activity modification, and anti-inflammatory medications may be sufficient.
- Persistent or unclear diagnosis: A superior cluneal nerve block is often the most informative next step, as it can both confirm the diagnosis and provide relief.
- Temporary relief after nerve block: This suggests the cluneal nerves are the primary pain source and may support repeating the injection or considering longer-acting treatments.
- Chronic or refractory pain: Procedures such as radiofrequency ablation (RFA) or selected regenerative therapies may be appropriate for longer-term relief.
Because symptoms of superior cluneal neuropathy often overlap with other causes of buttock pain, choosing the right treatment requires careful clinical evaluation. The goal is not simply to reduce pain, but to identify and treat the true source as precisely as possible.
If your symptoms have not responded to prior treatments or do not match your imaging findings, a more targeted evaluation may be warranted.
When the correct pain generator is identified, treatment becomes significantly more effective—and often much simpler.
Cluneal Neuropathy After Spine Surgery
Persistent pain after lumbar surgery does not always mean the surgery failed in the usual sense. Sometimes a different pain generator was present all along or emerged later. Superior cluneal nerve entrapment has been described as an important contributor to persistent low back pain after lumbar decompression, discectomy, and fusion in selected patients.
This matters because a patient with ongoing pain after surgery may still have a treatable source of symptoms, even if standard post-op imaging does not tell the full story.
Cluneal Neuropathy and Maigne Syndrome
Cluneal neuropathy also overlaps conceptually with other underrecognized causes of low back pain, including Maigne syndrome. Both conditions can cause pain patterns that seem confusing at first glance and both remind us that not all low back pain originates from discs, joints, or obvious imaging abnormalities.
For clinicians and patients alike, the lesson is simple: when the story does not fit neatly into a standard spine diagnosis, think wider.
Who Should Suspect Cluneal Neuropathy?
You or your clinician should think about cluneal neuropathy if you have:
- Localized pain near the iliac crest or upper buttock
- Back pain that worsens with walking, standing, twisting, or rolling in bed
- Tenderness at a very specific point over the posterior pelvis
- Pain that mimics sciatica but does not match imaging well
- Persistent pain after back surgery without a satisfying explanation
- Temporary pain relief after a targeted local injection
Why Accurate Diagnosis Matters
When cluneal neuropathy is missed, patients may be sent down the wrong hallway for months or years. They may be told their pain is nonspecific, muscular, or simply part of aging. Some undergo treatments that do not target the actual source.
When cluneal neuropathy is recognized, the picture often sharpens. The pain pattern makes more sense. The exam becomes more meaningful. The treatment becomes more precise. That is the difference between wandering through a fog and finally seeing the shoreline.
Dr. Amit Sharma & our minimally invasive pain & spine team.
Embedded Reference Article
For readers who want to review the published source article directly, the reference is embedded below:
If the embedded PDF does not load on your device, you can open it directly here:
Superior and Middle Cluneal Nerve Entrapment as a Cause of Low Back Pain
Additional related resources:
- Conditions Mimicking Spine Diseases
- Maigne Syndrome
- Superior Cluneal Nerve Entrapment
- Superior Cluneal Neuropathy
FAQ About Cluneal Neuropathy
What is cluneal neuropathy?
Cluneal neuropathy is pain caused by irritation or entrapment of the cluneal nerves, small sensory nerves that supply the lower back and buttock region.
Can cluneal neuropathy cause sciatica-like pain?
Yes. Cluneal neuropathy can mimic sciatica because the pain may radiate into the buttock, hip, groin, or leg even though the source is a peripheral sensory nerve rather than a spinal nerve root.
Does cluneal neuropathy show up on MRI?
Usually not. These nerves are very small, so routine MRI often does not directly show the problem. Diagnosis usually depends more on the history, physical exam, and response to a targeted nerve block.
How is cluneal neuropathy diagnosed?
Diagnosis is usually based on symptoms, a focal trigger point, reproduction of pain with pressure over the nerve, and relief after a diagnostic nerve block.
What treatments are available for cluneal neuropathy?
Treatment may include activity modification, physical therapy, medication, targeted nerve blocks, and in selected cases decompression or neurolysis of the entrapped nerve.
Is superior cluneal nerve entrapment the same thing as cluneal neuropathy?
Superior cluneal nerve entrapment is one common form of cluneal neuropathy. The term cluneal neuropathy is broader and may also include middle cluneal nerve irritation or entrapment.



