
Cervical Plexopathy: 7 Critical Facts for Faster Relief
What Is Cervical Plexopathy?
Cervical Plexopathy refers to an injury, inflammation, or compression of the cervical plexus—a network of nerves located in the neck that supplies sensation and motor control to parts of the neck, shoulders, and diaphragm. Patients with this condition may experience pain, numbness, tingling, or weakness in the neck, upper chest, or shoulder region.
Often mistaken for cervical radiculopathy or brachial plexus disorders, Cervical Plexopathy is less common but clinically significant due to its role in diaphragmatic control and proximal motor function. Accurate diagnosis is key for proper management.
Understanding Cervical Plexus Anatomy
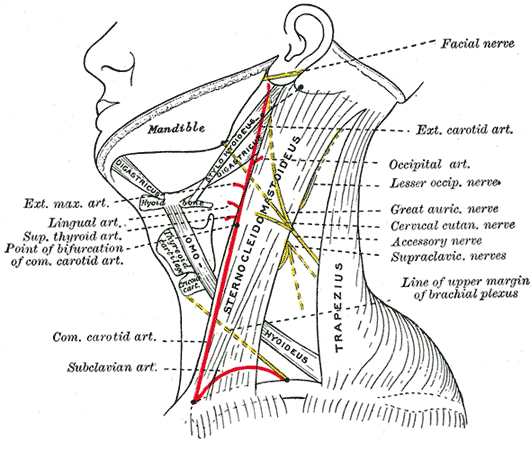
Think of the cervical plexus as a small nerve control panel located in the side of your neck. It’s made up of nerve fibers from the upper part of the spinal cord—specifically from cervical levels C1 through C4. These nerves exit the spinal column and join together like wires in a junction box to serve key areas of the body.
From this “nerve hub,” several important signals are sent out:
- Sensation: Some branches go to the skin on your neck, shoulders, collarbone, and around the ear. These help you feel touch, pain, or temperature in those areas.
- Movement: Other branches help control muscles that allow you to swallow, turn your neck, and breathe (including the phrenic nerve, which powers your diaphragm—the main breathing muscle).
This nerve network also communicates with deeper nerves in your shoulder (the brachial plexus) and with some cranial nerves that control facial functions. Because of its role in breathing and upper body control, damage to the cervical plexus can cause more than just neck pain—it may affect your ability to breathe deeply or lift your shoulder properly. This network also communicates with the cranial nerves and brachial plexus, making anatomical understanding crucial for both surgical and diagnostic interventions.
For an in-depth overview of spinal nerve organization, refer to our Neuroanatomy of the Spine guide.
How Does Cervical Plexopathy Differ from Brachial Plexopathy?
While both conditions involve nerve networks in the neck and upper chest, Cervical Plexopathy and Brachial Plexopathy affect different anatomical regions and cause distinct clinical symptoms.
The cervical plexus (C1–C4) primarily controls sensation in the neck and shoulder and helps power the diaphragm via the phrenic nerve. In contrast, the brachial plexus (C5–T1) governs motor and sensory function throughout the arm and hand. Differentiating these conditions is key for accurate diagnosis and treatment planning.
| Feature | Cervical Plexopathy | Brachial Plexopathy |
|---|---|---|
| Nerve roots involved | C1–C4 | C5–T1 |
| Area affected | Neck, shoulder, diaphragm | Shoulder, arm, forearm, hand |
| Sensory distribution | Lateral neck, jawline, upper chest | Entire upper limb |
| Key clinical features | Neck pain, breathing issues | Arm weakness, hand numbness |
| Common causes | Surgery, Parsonage-Turner, radiation | Trauma, tumors, thoracic outlet syndrome |
This comparison helps differentiate the likely source of symptoms and ensures patients receive the most appropriate diagnostic workup and treatment plan.
What Causes Cervical Plexopathy?
Cervical Plexopathy may result from a variety of causes including trauma, surgery, infection, or systemic illness. Common causes include:
- Direct trauma to the neck or clavicular region
- Complications from cervical spine or vascular surgeries
- Radiation therapy affecting neck structures
- Neuralgic amyotrophy (Parsonage-Turner Syndrome)
- Neoplasms compressing cervical nerve roots
- Diabetes and other metabolic disorders
In some cases, the cause remains idiopathic. Identifying the exact etiology helps determine the most effective treatment pathway.
Recognizing the Symptoms of Cervical Plexopathy
Symptoms vary depending on which nerve branches are affected. Patients typically present with:
- Sharp or burning pain in the side of the neck or upper shoulder
- Numbness over the lateral neck and upper chest
- Diaphragmatic dysfunction (in cases involving the phrenic nerve)
- Motor weakness in neck flexors or shoulder elevators
These symptoms can closely mimic radiculopathy, brachial plexopathy, or thoracic outlet syndrome. Electrodiagnostic studies and imaging help differentiate the diagnosis.
Parsonage-Turner Syndrome: A Key Cause of Cervical Plexopathy
Parsonage-Turner Syndrome (PTS), also called neuralgic amyotrophy, is a rare but distinctive condition often associated with Cervical Plexopathy. It typically begins with sudden, severe shoulder or neck pain, followed by progressive weakness and muscle atrophy in the shoulder girdle.
Though the exact cause is unclear, PTS has been linked to viral infections, vaccinations, surgeries, and autoimmune triggers. The brachial plexus is more commonly affected, but the cervical plexus—especially the phrenic nerve—may also be involved.
Diagnosis is clinical and supported by EMG, which may show patchy denervation. According to a 2018 review in Frontiers in Neurology, early corticosteroid therapy may reduce symptom duration in some cases, although recovery is often slow and incomplete.
How Is Cervical Plexopathy Diagnosed?
Diagnosing Cervical Plexopathy requires a careful combination of clinical examination, electrodiagnostic testing, and imaging studies. Your physician may perform:
- Neurological exam to assess motor weakness and sensory loss
- Diaphragmatic function tests if breathing issues are suspected
- Electromyography (EMG) to localize and characterize nerve damage
- MRI or CT to identify structural causes like tumors, trauma, or inflammation
- Blood tests to evaluate for metabolic or autoimmune contributors
EMG remains the gold standard for confirming cervical plexus involvement and differentiating it from radiculopathy or brachial plexopathy.
Treatment Options for Cervical Plexopathy
Treatment depends on the underlying cause, severity, and whether there’s ongoing nerve irritation. Options may include:
- Physical therapy: Restores muscle strength and range of motion
- Medication: Neuropathic pain agents like gabapentin or duloxetine
- Corticosteroids: Especially useful in autoimmune or Parsonage-Turner Syndrome cases
- Interventional pain procedures: Ultrasound-guided nerve blocks or hydrodissection
- Surgical decompression: For cases involving tumors, cysts, or persistent structural compression
At SpinePain Solutions, we offer a comprehensive diagnostic and treatment program tailored to nerve-related disorders including cervical plexus conditions.
Prognosis and Recovery
The outlook for Cervical Plexopathy varies based on cause and timing of diagnosis. Many cases resolve with conservative care, especially when identified early. However, some patients may experience long-term weakness or altered sensation.
Parsonage-Turner Syndrome, in particular, has a variable prognosis. While many recover function over 6 to 18 months, some may require assistive therapy or bracing. Studies in Muscle & Nerve show improved outcomes with early intervention and therapy.
Worried About Neck Pain or Arm Weakness?
If you’ve been diagnosed with or suspect Cervical Plexopathy, Dr. Amit Sharma offers advanced diagnostics and minimally invasive treatment options.
Frequently Asked Questions About Cervical Plexopathy
Is Cervical Plexopathy the same as cervical radiculopathy?
No. Cervical radiculopathy involves nerve roots near the spine, while Cervical Plexopathy affects the network of nerves in the side of the neck. They can cause similar symptoms but require different evaluation.
Can Cervical Plexopathy affect breathing?
Yes. If the phrenic nerve is involved, patients may experience shortness of breath, especially when lying down or exerting themselves.
What is the recovery time for Cervical Plexopathy?
Mild cases may recover in weeks, but more severe conditions like Parsonage-Turner Syndrome may take 6–18 months. Therapy and close follow-up are essential.



