
Disc Herniation – 7 Amazing Insights
If you’ve been told you have a disc herniation (often called a “herniated disc”), you’re in good company.
Disc herniation is one of the most frequent reasons adults between 30 and 60 develop chronic back pain, neck pain, and sciatica. Whether you’re dealing with sharp nerve pain, numbness, tingling, or a deep ache that just won’t let up, a disc herniation can disrupt nearly every part of daily life.
The encouraging news? Modern imaging, non-surgical spine care, and carefully selected regenerative medicine options have dramatically changed how specialists treat disc herniations—often avoiding major surgery altogether.
In this guide, we’ll walk through 7 game-changing insights about disc herniation treatment so you can understand your diagnosis, make sense of your MRI, and choose the safest and most effective path forward. We’ll start by reviewing what a spinal disc is and how disc problems—like bulges and herniations—develop over time.
What is a Disc Herniation?
The human spine is a remarkably engineered column that provides both strength and flexibility. Between most of the 33 vertebrae—especially in the neck, mid-back, and lower back—are soft cushions called intervertebral discs. These discs absorb shock and allow controlled movement, protecting the vertebrae, spinal cord, and nerve roots from everyday stresses.
Each disc has two key components:
- Annulus Fibrosus: A tough, fibrous outer ring that provides structure and containment.
- Nucleus Pulposus: A soft, gel-like center that distributes pressure and allows the disc to act like a shock absorber.
Throughout life, these discs are exposed to bending, twisting, lifting, and compressive forces. Over time—due to aging, repetitive strain, poor posture, trauma, smoking, or genetic factors—the annulus can weaken and become more vulnerable to injury.
What Happens in a Disc Herniation?
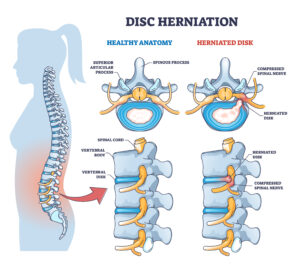 |
A disc herniation occurs when the outer layer of the disc (annulus fibrosus) develops a defect or tear, allowing the inner gel (nucleus pulposus) to push outward or leak through the weakened area.
This displaced material can crowd or compress nearby spinal nerves and trigger local inflammation, often causing pain, numbness, tingling, or muscle weakness. Study the image to get a clearer feel for the difference between a disc bulge and a disc herniation, and why their exact size and location matter. |
Disc Bulge vs Disc Herniation
Patients often hear both terms on MRI reports and wonder what they really mean.
A disc bulge is usually a more generalized, broad-based extension of the disc beyond its normal borders, while the outer ring remains intact—similar to a tire that is slightly over-expanded but not torn.
A disc herniation is more focal. There is a defect in the annulus, and the inner material pushes out or escapes through that tear. Herniations can be described as protrusions, extrusions, or even sequestrations, depending on how far the disc material has migrated.
Which is Worse?
Intuitively, people assume a herniated disc is always “worse” than a bulge. In reality, the most important question is not “How big is it?” but “Is it irritating or compressing a nerve that explains my exact symptoms?”
Some large disc bulges cause no symptoms at all, while a small focal disc herniation in a tight canal can cause significant pain, weakness, or numbness. The impact depends on:
- Which nerve or nerve roots are involved
- The precise location (central, paracentral, foraminal, or far-lateral)
- Your individual anatomy and degree of inflammation
What Causes a Disc to Herniate?
Common contributors to disc herniation include:
- Age-related disc degeneration and dehydration
- Repetitive bending, lifting, or twisting at work or during sports
- Sudden trauma, such as a fall or heavy lift with poor mechanics
- Poor posture and prolonged sitting, especially with weak core muscles
- Genetic predisposition to weaker connective tissue or early degeneration
Typical Symptoms of Disc Herniation
Not every herniated disc is symptomatic. When symptoms do occur, patients may notice:
- Localized neck or lower back pain
- Sciatica — sharp, shooting pain radiating from the back down the leg
- Arm pain or “electric” sensations with cervical disc herniation
- Numbness, tingling, or burning sensations in an arm or leg
- Muscle weakness in the shoulder, arm, hip, or foot
- Worsening pain when coughing, sneezing, or sitting for extended periods
Where Do Disc Herniations Most Commonly Occur?
Disc herniations most frequently involve the:
- Lumbar spine (lower back) — often causing leg pain or sciatica
- Cervical spine (neck) — often causing arm pain, numbness, or weakness
Herniations in the thoracic spine (mid-back) are less common, partly because the rib cage stabilizes this region and limits motion.
Are All Disc Herniations Serious?
No. Many herniated discs are discovered “by accident” on MRI in patients who have little or no symptoms. Even when pain is present, most cases improve with conservative, non-surgical care.
The goal is not to treat the MRI; it is to treat you. The presence of a disc herniation on imaging becomes meaningful when it clearly explains your symptoms and neurological findings.
For a deeper understanding of spinal anatomy, visit our full guide on Spine Anatomy or learn about Degenerative Disc Disease, another common disc-related condition.
How is a Disc Herniation Diagnosed?
One of the biggest misconceptions about disc herniation is that if it shows up on an MRI, it must be the cause of your pain. In reality, studies show many adults—especially over age 30—have disc bulges or herniations without any pain at all.
Hearing the words “disc herniation” or reading a concerning MRI report can be overwhelming. Our role is to replace fear and confusion with clear, honest guidance so you can make confident decisions.
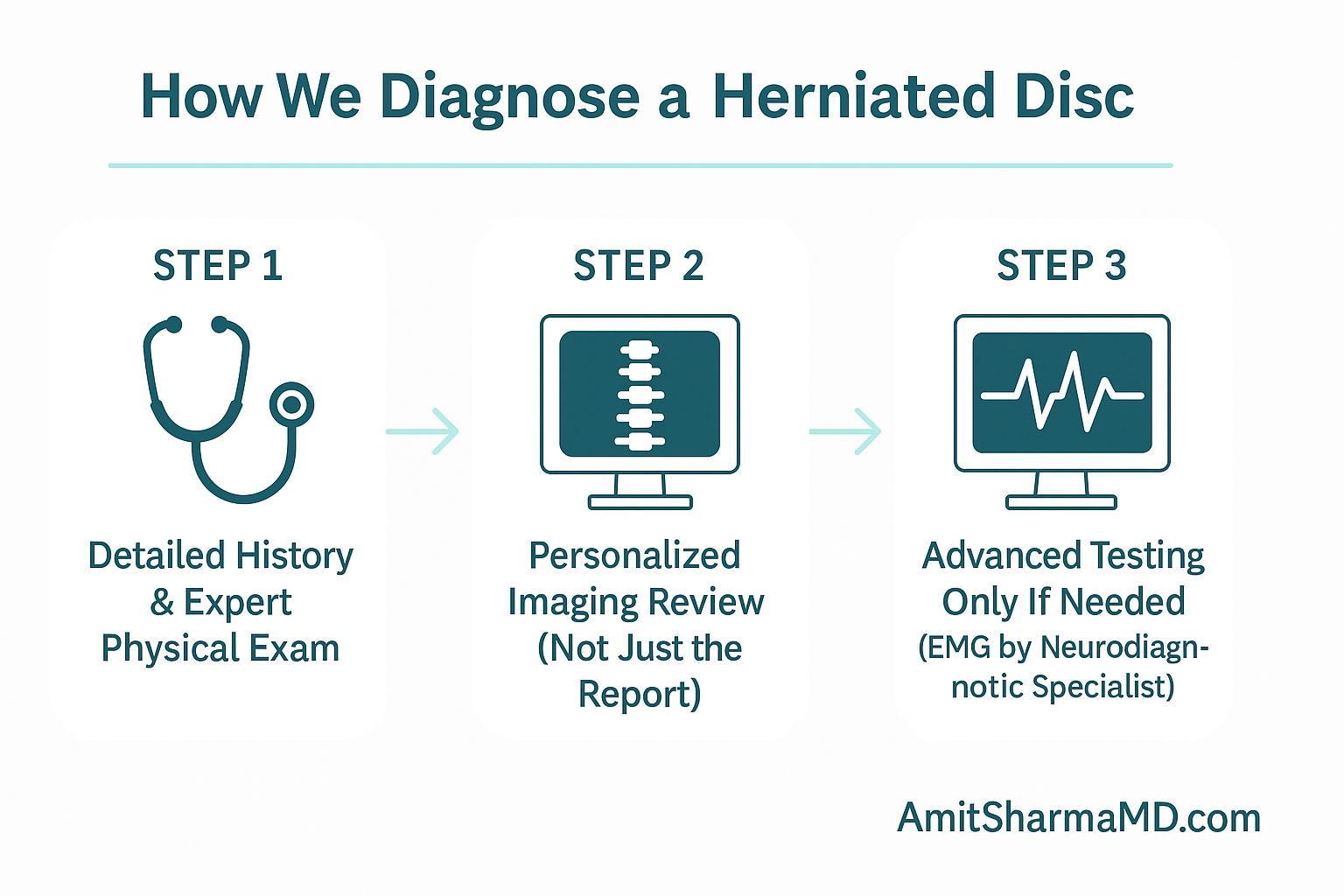
At SpinePain Solutions, we believe a disc herniation on a scan is only important if it lines up with your symptoms and exam. That’s why we:
- Personally review the MRI images (not just the written report)
- Take a detailed medical history and symptom map
- Perform a careful neurological and musculoskeletal examination
Only when all three match do we call a disc herniation clinically relevant.
Why MRI Findings Alone Aren’t Enough
Landmark research in the New England Journal of Medicine and other journals shows that more than half of people without back pain have disc abnormalities on MRI. In other words, a scan is a tool, not a verdict.
A thoughtful diagnosis integrates:
- Your story
- Your physical and neurological exam
- Your imaging and, when appropriate, advanced testing
Clinical Scenario 1: Sciatica from Lumbar Disc Herniation
A patient develops right-sided lower back pain radiating down the leg to the top of the foot. History suggests irritation of the L5 nerve root. On exam, we find:
- Positive Straight Leg Raise Test (SLRT)
- Numbness along the L5 dermatome
- Weakness in right Extensor Hallucis Longus (EHL)
- Altered reflexes
If the MRI shows a right L4–5 paracentral disc herniation contacting the L5 nerve root, that finding is highly relevant. A left-sided disc herniation in the same patient might be incidental.
Unsure Whether Your Disc Herniation is the Real Problem?
Many patients are told they have a disc herniation—but no one explains whether it truly explains their pain. At SpinePain Solutions, we offer expert evaluations and trusted second opinions to bring clarity to complex MRI reports.
Clinical Scenario 2: Cervical Disc Herniation with Arm Symptoms
A patient reports neck pain radiating into the right arm with tingling in the thumb and index finger. Examination reveals:
- Reduced biceps reflex
- Sensory changes in the C6 dermatome
- Weakness with elbow flexion
- Positive Spurling’s test
The MRI shows a right C5–C6 disc herniation compressing the C6 nerve root—making this disc herniation clinically significant.
Clinical Scenario 3: Incidental Thoracic Disc Herniation
A patient has an MRI after minor trauma and is found to have a small thoracic disc herniation at T7–T8, but no nerve symptoms. In this case, the disc herniation is an incidental finding, and no intervention is needed.
Advanced Diagnostics—Only When Needed
In select complex situations, we may recommend tests like EMG (Electromyography) to evaluate nerve function. However, EMG is not required for most patients and has important limitations.
When EMG is truly appropriate, we refer to a neurologist with formal specialty certification in neurodiagnostics—a physician who is board-certified in neurology with advanced expertise in electrodiagnostic medicine (EMG, EEG, and related modalities). This ensures that the results are precise and integrated thoughtfully into your treatment plan, rather than driving unnecessary procedures.
Second Opinions for Disc Herniation
Even if you don’t choose us for long-term care—due to insurance, distance, or personal preference—we are happy to provide comprehensive second opinions on disc herniation and related conditions. A careful, balanced review can prevent unnecessary spine surgery and open doors to safer, less invasive options.
For patients across Long Island seeking clear answers about disc herniation, back pain, or neck pain, SpinePain Solutions is dedicated to delivering precision diagnostics and personalized, evidence-based care.
Disc Herniation Treatment Options
A diagnosis of disc herniation does not automatically mean you need surgery. In fact, most disc herniations can be treated successfully with advanced non-surgical and minimally invasive interventions—when you’re evaluated by a specialist who understands when surgery is truly necessary.
At SpinePain Solutions, we use a comprehensive approach designed to relieve pain, restore function, and help you avoid unnecessary procedures whenever possible.
Conservative Treatments: The First Line
For many patients, the first phase of treatment focuses on reducing pain and inflammation and supporting natural healing:
- Activity Modification: Avoiding provocative positions while staying gently active.
- Physical Therapy: Customized core-strengthening and stabilization programs to reduce nerve irritation.
- Medications: Judicious use of anti-inflammatories, nerve-modulating agents, or muscle relaxants.
- Chiropractic Care: When appropriate, we collaborate closely with trusted chiropractors across Long Island to coordinate safe, patient-centered care.
Precision Interventional Spine Care
When conservative care does not provide sufficient relief, we can precisely target the disc herniation and irritated nerve with image-guided procedures:
- Transforaminal Epidural Steroid Injections (TF ESI): Delivering medication directly into the ventral epidural space, where disc herniations typically compress nerve roots. This approach is often more effective than traditional “blind” or less targeted injections.
- Selective Nerve Root Blocks: Used both diagnostically and therapeutically to confirm which nerve is involved and relieve radicular pain.
- Versa-Kath Directed Epidural Injections: Exclusively performed by Dr. Sharma on Long Island, this technique allows safe, effective treatment even at challenging cervical levels such as C2–3 and C3–4, where very few specialists are comfortable operating.
Advanced Options for Chronic Radiculopathy
For patients with persistent nerve pain from disc herniation—especially when surgery has failed or is not clearly indicated—we may consider:
- Pulsed Radiofrequency Ablation (PRF) of the Dorsal Root Ganglion (DRG): A non-destructive way to modulate chronic nerve pain signals.
- DRG Stimulation: A specialized form of neuromodulation for refractory radicular pain syndromes.
Regenerative Medicine: Emerging Therapies
For select patients, we are exploring biologic therapies such as Platelet-Rich Plasma (PRP), stem cell–based treatments, and other regenerative approaches, particularly for disc-related pain. These treatments aim to support the body’s natural repair processes.
Disclaimer: Regenerative medicine treatments are considered investigational and are not FDA-approved specifically for disc herniation. Individual results vary, and these options should be discussed in detail with your specialist.
Learn more through our regenerative medicine division, Bloom Infusions & Wellness.
Minimally Invasive Spine Procedures
When treatment beyond injections is needed, we focus on techniques that minimize tissue trauma and recovery time:
- Transforaminal Full Endoscopic Discectomy: A state-of-the-art outpatient procedure performed through a tiny incision with camera guidance to remove the offending disc herniation while preserving as much normal tissue as possible.
Making Sure Surgery is Truly Necessary
Spine surgery can be life-changing when used appropriately for disc herniation with severe or progressive neurological compromise. However, surgery is sometimes recommended based heavily on MRI findings, without careful correlation to symptoms and exam.
Research has shown that the United States performs significantly more spine surgeries than many other developed countries—at least 40% more in some analyses, and in certain comparisons more than five times the rate seen in England and Scotland. [PubMed Study]
Other work comparing New York to Ontario found elective spine surgery rates were approximately 300% higher in New York. [PMC Article]
Patients sometimes arrive after hearing alarming statements such as:
- “This is the worst disc herniation I’ve ever seen.”
- “You could be paralyzed without immediate surgery.”
- “We don’t know how you’re not already in a wheelchair.”
In many of these cases, the disc herniation seen on MRI is not clearly correlated with their symptoms or neurological exam.
Our mission at SpinePain Solutions is to offer a thorough, balanced evaluation to determine whether non-surgical or minimally invasive options can address the disc herniation before considering operative intervention.
Even neurosurgical literature generally agrees that clear indications for surgery in disc herniation include:
- Severe or progressive neurological deficits (such as significant weakness)
- Pain that remains disabling despite appropriately delivered conservative care
- Emergencies such as cauda equina syndrome
That’s why we reserve time for urgent appointments—often within 24–72 hours—to provide second opinions and help patients avoid unnecessary operations.
When Surgery is the Right Choice
In the relatively small percentage of disc herniation cases where surgery is appropriate, we work closely with select spine surgeons who share our patient-first, evidence-based approach. Our goal is to ensure you receive clear counseling on risks, benefits, and alternatives.
Why Patients Choose SpinePain Solutions for Disc Herniation Care
- Expertise in advanced interventional spine techniques
- Exclusive provider of Versa-Kath procedures on Long Island
- Minimally invasive endoscopic discectomy experience
- Access to emerging regenerative therapies through Bloom Infusions & Wellness
- Rapid second opinions to help avoid unnecessary spine surgery
- Personalized, ethical care focused on long-term function and quality of life
Get Clarity on Your Disc Herniation Before Saying “Yes” to Surgery
If you’ve been told you need spine surgery because of a disc herniation—or you’re simply unsure about your options—schedule a consultation with SpinePain Solutions. We’ll carefully review your MRI, exam, and history to explore all non-surgical and minimally invasive solutions first.
When to See a Spine Specialist for Disc Herniation
Mild neck or back pain often improves over time. However, certain symptoms suggest that a disc herniation—or another spinal condition—should be evaluated promptly. You should seek professional care if you notice:
- Pain lasting more than 2–3 weeks despite rest and basic self-care
- Numbness, tingling, or weakness in an arm or leg
- Difficulty performing work duties, household tasks, or sleeping due to pain
- Loss of bowel or bladder control — seek emergency medical attention
At SpinePain Solutions, we provide detailed evaluations and customized treatment plans across our convenient locations in Commack, Bay Shore, Bethpage, and Huntington, NY—serving patients throughout Long Island.
Conclusion: Disc Herniation Relief Without Rushing to Surgery
A disc herniation diagnosis does not mean your life has to shrink around your pain—or that your only option is major surgery. With accurate diagnosis, targeted interventional treatments, and carefully selected regenerative therapies, most patients can achieve meaningful, lasting relief without open spine surgery.
If you’re experiencing back pain, neck pain, or sciatica symptoms and have been told you have a herniated disc, don’t delay evaluation. A thoughtful, early plan can prevent worsening nerve damage and help you return to safe, confident activity.
Take the First Step Toward Disc Herniation Relief
Schedule Appointment
Same-day and urgent appointments are often available so you can get the answers—and relief—you deserve.
Frequently Asked Questions:
What is the fastest way to feel better with a disc herniation?
There’s no instant cure, but combining activity modification, targeted physical therapy, and—when appropriate—precise interventional treatments can speed recovery and reduce nerve irritation.
Do all disc herniations need surgery?
No. The majority of disc herniations improve without surgery. Many patients do well with a tailored combination of physical therapy, medication, and image-guided injections.
Can a disc herniation heal on its own?
Yes. Many disc herniations gradually improve over weeks to months as inflammation decreases and the body resorbs some of the disc material. Persistent or worsening symptoms should be evaluated.
How do I know if my disc herniation is serious?
Red flags include severe or rapidly worsening pain, weakness, or changes in bowel or bladder control. These may indicate significant nerve compression and require urgent medical attention.
What activities should I avoid with a disc herniation?
Avoid heavy lifting, repetitive bending/twisting, and prolonged sitting—especially without breaks. Guided, gentle activity is generally better than complete bed rest.
Is walking good for a disc herniation?
Light walking is often beneficial. It helps maintain spinal mobility, improves circulation, and can reduce stiffness when introduced gradually and safely.
What is the best non-surgical treatment for disc herniation?
There is no single “best” option. The ideal plan may include physical therapy, transforaminal epidural injections, selective nerve root blocks, and—when appropriate—regenerative medicine or minimally invasive procedures.
When should I see a doctor for disc herniation?
If symptoms last more than 2–3 weeks, if you develop numbness, tingling, weakness, or shooting pain down an arm or leg, or if your pain disrupts sleep and daily function, it’s time to see a spine specialist for a thorough evaluation and personalized treatment plan.



