
Deep Gluteal Syndrome: When Buttock Pain Has Many Names
- Posted on: Jun 20 2026
Deep gluteal syndrome (DGS) is one of the most quietly frustrating diagnoses in pain medicine — not because it’s rare, but because almost nobody calls it by the same name twice. A physical therapist may call it piriformis syndrome. A chiropractor may call it an SI joint problem. A neurologist may suspect a pinched nerve or neuralgia. A spine specialist may chalk it up to referred pain from the lumbar spine. Patients end up with four different opinions, four different treatment plans, and often, no lasting relief — because the structures these specialists are each examining can genuinely overlap, and the actual source of the pain is frequently none of them in isolation.
This article explains what DGS actually is, why it gets mistaken for so many other conditions, how it’s properly diagnosed, and what the evidence says about treatment. For the bigger picture of everything that can cause pain in this region, see our buttock pain overview, which maps DGS alongside its most common mimics.
Why the Same Buttock Pain Gets Five Different Diagnoses
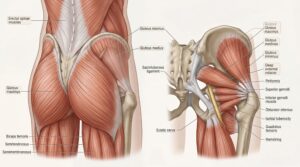 Deep, aching buttock pain — sometimes radiating down the back of the thigh — sits at a genuine anatomical crossroads. The sciatic nerve passes directly beneath (and occasionally through) the piriformis muscle, runs near the obturator internus and gemelli muscles, skims past the ischial tuberosity where the hamstrings attach, and lies just inferior to the sacroiliac joint and lumbosacral plexus. A problem in almost any of these neighboring structures can produce strikingly similar symptoms.
Deep, aching buttock pain — sometimes radiating down the back of the thigh — sits at a genuine anatomical crossroads. The sciatic nerve passes directly beneath (and occasionally through) the piriformis muscle, runs near the obturator internus and gemelli muscles, skims past the ischial tuberosity where the hamstrings attach, and lies just inferior to the sacroiliac joint and lumbosacral plexus. A problem in almost any of these neighboring structures can produce strikingly similar symptoms.
In one of the most cited diagnostic series on sciatic-type buttock pain, researchers reviewed 239 patients and found that piriformis-related sciatic nerve entrapment accounted for the majority of cases, but distal foraminal entrapment, ischial tunnel entrapment, pudendal nerve involvement, sacroiliac joint inflammation, and discogenic referred pain each made up meaningful slices of the remainder (Hicks et al., StatPearls, citing Filler et al.). That’s the clinical reality behind the joke clinicians sometimes make about this condition: depending on whose exam table you’re on, you may walk away with a completely different diagnosis — and each specialist may be partially right.
Dr. Amit Sharma & our minimally invasive pain & spine team.
What Is Deep Gluteal Syndrome?
DGS is the umbrella term for non-discogenic entrapment or irritation of the sciatic nerve as it passes through the deep gluteal space — the region beneath the gluteus maximus, bounded by the piriformis, obturator internus, gemelli, quadratus femoris, and the proximal hamstring origin. The defining feature is that the pain does not come from the spine itself; it comes from soft-tissue compression or irritation of the nerve outside the spinal canal.
Reported prevalence estimates vary widely — from roughly 5% to over a third of patients evaluated for sciatica-type symptoms — largely because the condition has historically been under-recognized and inconsistently defined (Kizaki et al., narrative review, 2025). A 2023 systematic review pooling 853 clinically diagnosed cases proposed a clearer working definition: a non-discogenic sciatic nerve disorder caused specifically by entrapment within the deep gluteal space, diagnosed through a combination of history, physical exam, imaging, response to diagnostic injection, and nerve-specific electrodiagnostic testing (Park et al., systematic review).
Beyond the Piriformis: The Other Structures That Can Trap the Sciatic Nerve
Piriformis syndrome is the best-known cause of DGS, and it remains the single most common one. The piriformis can compress the sciatic nerve through outright hypertrophy, dynamic entrapment during certain hip movements, an anatomically anomalous nerve path, or scarring from prior trauma or surgery (summary of the orthopedic literature).
But “piriformis syndrome” has, somewhat unhelpfully, become a catch-all label applied to several distinct problems that happen to live in the same neighborhood. Recognized causes of DGS besides true piriformis entrapment include:
- Obturator internus/gemelli syndrome — entrapment at the twin gemelli muscles and their shared tendon
- Ischiofemoral impingement — narrowing of the space between the ischium and lesser trochanter
- Quadratus femoris pathology — strain or tearing near its attachment at the ischial tuberosity
- Proximal hamstring tendinopathy or tears, which can irritate the adjacent nerve
- Fibrovascular bands and anomalous vessels crossing the nerve
- Less commonly, pelvic floor or gynecologic/urologic sources referring pain into the same region
A point worth being clear about: several of these — proximal hamstring tendinopathy and ischiofemoral impingement in particular — can also occur as standalone conditions that produce buttock pain without entrapping the sciatic nerve at all. In other words, they’re sometimes a cause of DGS and sometimes their own diagnosis. Our buttock pain overview lays out the full differential, including these and other mimics like ischial bursitis and coccydynia.
A 2021 review notes that the all-purpose “piriformis syndrome” label has, in practice, absorbed several of these genuinely separate diagnoses, and argues for a more precise, structure-specific diagnostic approach (Martin et al., deep gluteal space problems). This is exactly why a PT who tests piriformis flexibility, a chiropractor who assesses SI joint mechanics, and a spine physician evaluating for referred or radicular pain can each find something real — and still all be only partially correct.
How DGS Differs From SI Joint Pain, Discogenic Pain, and True Radiculopathy
Getting the diagnosis right matters because the treatments diverge sharply. A patient treated for SI joint dysfunction when the actual problem is sciatic nerve entrapment at the piriformis — or vice versa — will predictably plateau.
DGS (sciatic nerve entrapment): Deep, often burning or electric buttock pain that radiates down the posterior thigh, frequently worsened by prolonged sitting, and sometimes accompanied by numbness or tingling along the sciatic distribution. Lumbar imaging is typically unremarkable or shows findings that don’t explain the symptom pattern.
SI joint pain: Pain centered more directly over the sacral dimple, usually without a clear nerve-pattern radiation below the knee, and reproduced by SI joint provocation maneuvers (distraction, compression, thigh thrust, Gaenslen’s, sacral thrust) rather than sciatic nerve tension tests. Our Sciatica vs. SI Joint Pain guide walks through this distinction in more detail.
Lumbar discogenic pain or true radiculopathy: Pain that follows a specific dermatomal pattern tied to a nerve root level, often with a positive straight-leg raise test and corresponding findings on lumbar MRI — a herniation or stenosis at the level that matches the symptoms.
Superior cluneal nerve entrapment: A frequently overlooked source of upper-buttock and iliac-crest pain that can mimic both SI joint pain and facet joint pain; see our guides on cluneal neuropathy and superior cluneal nerve entrapment if your pain sits higher, near the belt line, rather than centered in the deep buttock.
None of these patterns is diagnostic in isolation, and overlap is common — which is precisely why DGS is so often missed, partially treated, or treated as the wrong condition entirely.
How DGS Is Diagnosed
Diagnosis starts with ruling out a spinal cause. Once lumbar pathology has been reasonably excluded through history, exam, and review of existing imaging, attention turns specifically to the deep gluteal space. A focused evaluation typically includes:
- Provocative maneuvers that reproduce sciatic-type pain with resisted hip external rotation or passive internal rotation and flexion (commonly grouped under the FAIR test and related seated piriformis stretch maneuvers).
- A detailed history of trauma, prior hip or spine surgery, prolonged sitting (sometimes still informally called “wallet sciatica”), or activities involving repetitive hip rotation.
- Advanced imaging when conservative care hasn’t helped — MR neurography or dynamic ultrasound can visualize the sciatic nerve directly and may show signal change, nerve swelling, or compression at a specific structure, helping distinguish piriformis entrapment from obturator internus, ischiofemoral, or hamstring-related causes (Kurková et al., 2025).
- Response to a diagnostic, image-guided injection at the suspected site — if precisely placed local anesthetic substantially relieves the pain, it strongly supports that structure as the true pain generator, the same logic used in piriformis injections and other diagnostic blocks throughout spine and pain medicine.
- Nerve-specific testing, such as electromyography, in select cases where motor involvement or a more diffuse neuropathic process needs to be clarified.
Treatment Options: From Physical Therapy to Image-Guided Nerve Hydrodissection
As with most pain generators discussed on this site, treatment for DGS follows a stepwise approach rather than jumping straight to a procedure.
Conservative care first. A structured course of physical therapy — specifically targeting piriformis and external rotator flexibility, sciatic nerve glides, and hip circumduction — combined with activity modification and anti-inflammatory medication is the appropriate first step for most patients, generally continued for at least four to six weeks before escalating (StatPearls review). It’s worth being honest that generic “core strengthening” or non-specific stretching protocols often underperform compared to therapy that’s actually targeted at nerve mobility and the specific entrapment site.
Ultrasound-guided nerve hydrodissection. For patients who don’t improve with conservative care, image-guided hydrodissection — injecting a low-volume mixture (commonly dextrose, local anesthetic, and a small dose of corticosteroid) around the sciatic nerve to mechanically free it from surrounding adhesions — has reasonable supporting evidence.
A 2024 case series of 53 patients followed for three to nineteen months found favorable outcomes (defined as ≥50% pain reduction) in 73.6% of patients at one week, declining somewhat to 71.7% at one month, 64.2% at three months, and 62.3% at final follow-up (Yen et al., Diagnostics, 2024). In intellectual honesty, that’s a meaningful but gradually fading effect for many patients with a single injection — which is consistent with what’s reported elsewhere in the literature, where some patients require up to three injections to achieve a lasting result. Side effects in that series were limited to transient dizziness in a small minority, with no nerve or vessel injury reported.
Endoscopic sciatic nerve decompression. For patients with a clearly identified anatomical entrapment who haven’t responded to physical therapy and injection-based care, endoscopic release of the entrapping structure is a well-supported option. A 2024 systematic review concluded that endoscopic treatment of sciatic nerve entrapment in DGS is effective and safe when conservative therapy has failed, offering meaningful pain relief and functional improvement with a low complication rate (systematic review, Eur J Orthop Surg Traumatol, 2024). This is reserved for genuinely refractory cases and follows the same diagnostic-confirmation principle used throughout interventional spine and pain care: don’t operate on a structure that hasn’t been confirmed as the actual pain generator.
When It’s Time to Ask for a Second Look
If you’ve been told you have “piriformis syndrome” or “SI joint pain” and treatment for one hasn’t moved the needle after a genuine, structured course of therapy, it doesn’t necessarily mean the original clinician was wrong — it may mean only part of the picture was examined. DGS deserves consideration any time deep buttock pain with posterior thigh radiation hasn’t responded to a focused trial of physical therapy, especially when lumbar imaging doesn’t clearly explain the symptoms.
A comprehensive evaluation that specifically maps the deep gluteal space — rather than treating the first plausible diagnosis — is often the missing step.
Dr. Amit Sharma & our minimally invasive pain & spine team.
Frequently Asked Questions
What is deep gluteal syndrome?
Deep gluteal syndrome (DGS) is non-discogenic entrapment or irritation of the sciatic nerve as it passes through the deep gluteal space beneath the gluteus maximus — an area that includes the piriformis, obturator internus, gemelli, quadratus femoris, and the proximal hamstring origin. It causes deep buttock pain that often radiates down the back of the thigh.
Is deep gluteal syndrome the same as piriformis syndrome?
Not exactly. Piriformis syndrome is the most common cause of DGS, but it’s only one of several possible causes. Obturator internus/gemelli entrapment, ischiofemoral impingement, hamstring tendinopathy, and fibrovascular bands can all produce a very similar pain pattern.
How is DGS different from SI joint pain?
SI joint pain is typically centered more directly over the sacral dimple and doesn’t usually follow a sciatic nerve pattern below the knee. DGS more often produces burning or electric pain radiating down the posterior thigh and is reproduced by sciatic nerve tension and hip rotation maneuvers rather than SI joint provocation tests.
Can an MRI diagnose DGS?
Standard lumbar MRI is mainly useful for ruling out a spinal cause. Specialized imaging — MR neurography or dynamic ultrasound of the sciatic nerve in the gluteal space — can sometimes directly visualize the entrapment, but diagnosis usually relies on a combination of history, physical exam, and response to a diagnostic injection.
What is sciatic nerve hydrodissection?
It’s an ultrasound-guided injection technique that uses fluid to mechanically separate the sciatic nerve from surrounding tissue that’s compressing or tethering it. Case-series data shows meaningful pain reduction in roughly two-thirds of patients at follow-up, though the effect can fade over time and some patients need more than one injection.
Is surgery ever needed for DGS?
Surgery is reserved for patients with a clearly confirmed entrapment who haven’t responded to physical therapy and image-guided injections. Endoscopic sciatic nerve decompression has good supporting evidence for safety and effectiveness in appropriately selected, refractory cases.
References
- Hicks BL, Lam JC, Varacallo M. Piriformis Syndrome. StatPearls. NCBI Bookshelf
- Filler AG, et al. Diagnosis and treatment of sciatic nerve entrapment in DGS (239-patient diagnostic series). PMC
- Beyond Nerve Entrapment: A Narrative Review of Muscle–Tendon Pathologies in DGS. Diagnostics 2025. MDPI
- Park JW, et al. DGS as a non-discogenic sciatic nerve disorder with entrapment in the deep gluteal space: a systematic review (853 patients). ResearchGate
- Martin HD, et al. Deep gluteal space problems: piriformis syndrome, ischiofemoral impingement and sciatic nerve release. Muscles Ligaments Tendons J. PMC
- Kurková S, et al. Exploring non-invasive diagnostic tools for DGS. Quant Imaging Med Surg. 2025. PMC
- Yen YS, Lin CH, Chiang CH, Wu CY. Ultrasound-guided sciatic nerve hydrodissection in DGS: a case-series study. Diagnostics 2024;14(7):757. PubMed
- Endoscopy for sciatic nerve entrapment in DGS: a systematic review. Eur J Orthop Surg Traumatol. 2024. PubMed
- Endoscopic sciatic neurolysis for DGS: a systematic review. PMC
- Cleveland Clinic. Piriformis Syndrome. Cleveland Clinic
Tagged with: Buttock Pain
Posted in: Special Report



