Two Devices, One Nerve, No Head-to-Head Data: Navigating the OptaBlate vs. Intracept Decision
- Posted on: May 29 2026
By Amit Sharma, MD
Interventional Pain Management | Pain Management and Spine Care
Introduction
Basivertebral nerve ablation has earned its place in the interventional pain toolkit. The evidence base is real, the patient selection criteria are well-defined, and for appropriately chosen patients with Modic Type 1 or 2 changes and refractory vertebrogenic low back pain, the outcomes are genuinely meaningful. That conversation is largely settled.
What is not settled is which device, and which protocol, best serves our patients in 2026.
I have performed BVN ablation using both the Intracept system (Boston Scientific) and the OptaBlate system (Stryker), and I want to offer an honest proceduralist’s analysis — not a promotional piece for either company, and not a recitation of manufacturer claims. Physicians deserve a clearer framework for this decision than either company’s sales team will provide.
The Evidence Landscape — Starting With Intellectual Honesty
Any fair comparison must begin here: the published evidence base belongs entirely to Intracept. Two Level I randomized controlled trials — the SMART sham-controlled trial and the INTRACEPT trial — with durability data extending to five years, form the scientific foundation on which BVN ablation as a category was built. The ASPN best practice guidelines reference this body of work specifically.
OptaBlate received FDA 510(k) clearance in May 2025. It is walking a road that Intracept spent years and significant resources constructing. When Stryker references long-term BVN ablation outcomes in its materials, it is citing Intracept’s trials — not its own. That is not a criticism; it is simply the current state of the evidence, and physicians should understand it clearly.
This does not mean OptaBlate is inferior. It means we do not yet know.
What We Actually Do in Practice — Protocol Reality
The 85°C/15-minute Intracept protocol that anchors the published trials has largely been replaced in private practice by the 7-minute cycle. The longer protocol is increasingly reserved for suboptimal probe positioning. This is an important acknowledgment: the real-world practice of BVN ablation has already diverged from its own evidence base, and that divergence is broadly accepted within the interventional pain community.
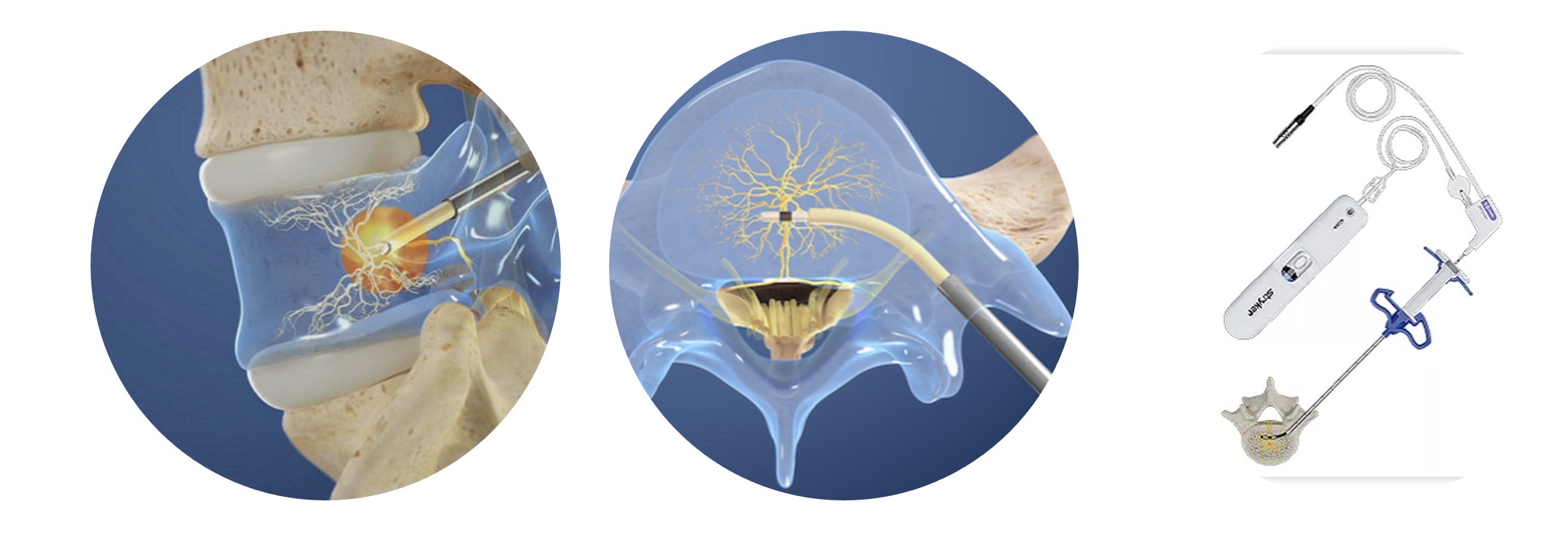
OptaBlate enters this environment running a protocol of 95°C for 7 minutes — a higher temperature target than either Intracept option, delivered through a bipolar probe with an integrated Microinfuser technology designed to maintain perielectrode hydration throughout the ablation cycle.
The comparison that matters in daily practice is therefore not OptaBlate versus the published literature. It is 95°C/7 minutes versus 75°C/7 minutes — same duration, meaningfully different temperature, different impedance management strategies.
The Physics — What Temperature Actually Does at Equal Duration
When duration is held constant, temperature becomes the dominant determinant of lesion size. The mechanism is well understood: RF energy creates a zone of resistive heating immediately around the electrode. Beyond that zone, tissue destruction depends on conductive heat spreading outward. The critical threshold for irreversible neural injury is approximately 50°C. The further the 50°C isotherm extends from the probe tip, the larger the effective lesion.
At 95°C versus 75°C at equal duration, the higher temperature drives that isotherm meaningfully further into surrounding tissue. In principle, OptaBlate’s protocol should produce a larger lesion radius than Intracept’s 7-minute option.
However, there is a significant caveat that cannot be dismissed. At temperatures above roughly 80°C, perielectrode tissue desiccation begins — charring that causes a sharp rise in local impedance, which progressively chokes energy delivery. The generator may report target temperature maintained while actual power output has dropped substantially partway through the cycle. The lesion stops growing while the timer keeps running.
This is precisely where the Microinfuser becomes mechanistically critical, not merely a marketing feature. By continuously hydrating the perielectrode environment, it prevents the resistance spike that would otherwise limit energy delivery at 95°C. The physics of this approach are sound.
The unanswered question is whether it performs as designed inside cancellous vertebral bone — a heterogeneous environment of variable mineral density, sinusoidal vascular channels, and marrow fat — rather than the soft tissue models on which the technology was largely validated. That is not a trivial distinction, and the answer will only come from independent outcomes data collected over time.
The Proceduralist’s Real Problem — Geometric Uncertainty
Here is an insight that neither company’s marketing addresses directly, because neither benefits from admitting it: we cannot see the basivertebral nerve.
BVN targeting is probabilistic. We work from fluoroscopic landmarks, pre-procedure MRI planning, and established anatomical relationships. The curved cannula does not always land exactly where intended. Bone density varies. Patient anatomy varies. The BVN’s precise location within the posterior vertebral body varies.
In this context, a larger lesion radius is not merely an academic advantage. If OptaBlate’s 95°C protocol reliably produces a larger destruction zone — and if the Microinfuser successfully sustains that energy delivery throughout the full 7-minute cycle in intraosseous bone — then it may offer a meaningful margin of geometric tolerance. A probe placement that is slightly off-target but surrounded by a larger thermal footprint may still capture the BVN completely, where a smaller lesion would not.
This is a clinically important hypothesis. It is not yet proven.
The transient radiculopathy occasionally observed following OptaBlate procedures is likely a reflection of this same phenomenon — thermal spread reaching periforaminal structures. That it typically resolves within 2 to 3 weeks is consistent with neurapraxia from thermal edema rather than structural nerve injury, and is broadly reassuring. But it also serves as a reminder that a larger lesion is not unconditionally better, and that the margin between therapeutic and collateral spread is finite.
What Boston Scientific Will Argue — And Where It Has a Point
Intracept’s generator incorporates real-time power management designed to regulate temperature and ramp rate throughout the ablation cycle. Boston Scientific will reasonably argue that this provides adequate impedance management at their target temperatures, making the Microinfuser’s advantage less relevant within their operating range.
They are not wrong that 75°C sits below the aggressive desiccation threshold where impedance becomes a dominant limiting factor. Their system was engineered around that temperature range and performs predictably within it.
The legitimate question is whether 75°C for 7 minutes produces sufficient thermal dose at the lesion margin to ensure permanent, rather than temporary, neural disruption. Neurapraxia — temporary conduction block — resolves. Axonotmesis does not. The difference between a durable outcome and a 6-month partial responder may lie at the margin of the lesion, where the thermal gradient is steepest and the distinction between reversible and irreversible injury is narrowest.
This is not a settled question for either device at the 7-minute duration.
A Framework for the Current Decision
In the absence of head-to-head data, here is how I think about the choice:
The evidence-based default remains Intracept. Its track record is real, its safety profile is documented at scale, and its long-term durability is established. For straightforward anatomy, optimal probe placement, and patients where procedural conservatism is appropriate, it remains the defensible choice.
OptaBlate’s higher temperature protocol is physically coherent and mechanistically interesting. Its potential advantage — larger lesion with maintained energy delivery — is a rational hypothesis, not a confirmed outcome. For experienced proceduralists comfortable with the system, it represents a reasonable clinical option, particularly where anatomical complexity makes geometric tolerance more valuable. The transient radiculopathy risk should be discussed with patients pre-procedure.
What neither device has yet is independent, non-industry-funded outcomes data at 12 and 24 months comparing the two protocols directly. Until that exists, every proceduralist using OptaBlate is, in a meaningful sense, contributing to the evidence base whether they intend to or not.
Conclusion
BVN ablation works. The mechanism is sound, the patient selection criteria are well established, and for the right patient it offers durable relief that conservative care cannot match. That is not in question.
What remains genuinely open is whether a higher-temperature, impedance-managed protocol produces outcomes that are superior, equivalent, or situationally better than the established lower-temperature approach. The physics suggest OptaBlate’s protocol should produce a larger, more geometrically tolerant lesion — if its Microinfuser performs as claimed in intraosseous bone. Whether that translates into better or more durable clinical outcomes is a question that only independent longitudinal data will answer.
Intracept built the foundation. OptaBlate is making an interesting argument about how to build on it. Our patients deserve us to keep asking the hard questions rather than simply accepting either company’s narrative.
Dr. Amit Sharma is an interventional pain management physician practicing at four locations on Long Island, New York, with fellowship training from Johns Hopkins and faculty affiliation at Columbia University. He performs BVN ablation using both the Intracept and OptaBlate systems.
Tagged with: basivertebral nerve ablation, Intracept, Modic Changes, OptaBlate, Vertebrogenic Pain
Posted in: Special Report



