Pedicle: The #1 Proven Anchor & The Gateway
What is a pedicle in the spine?
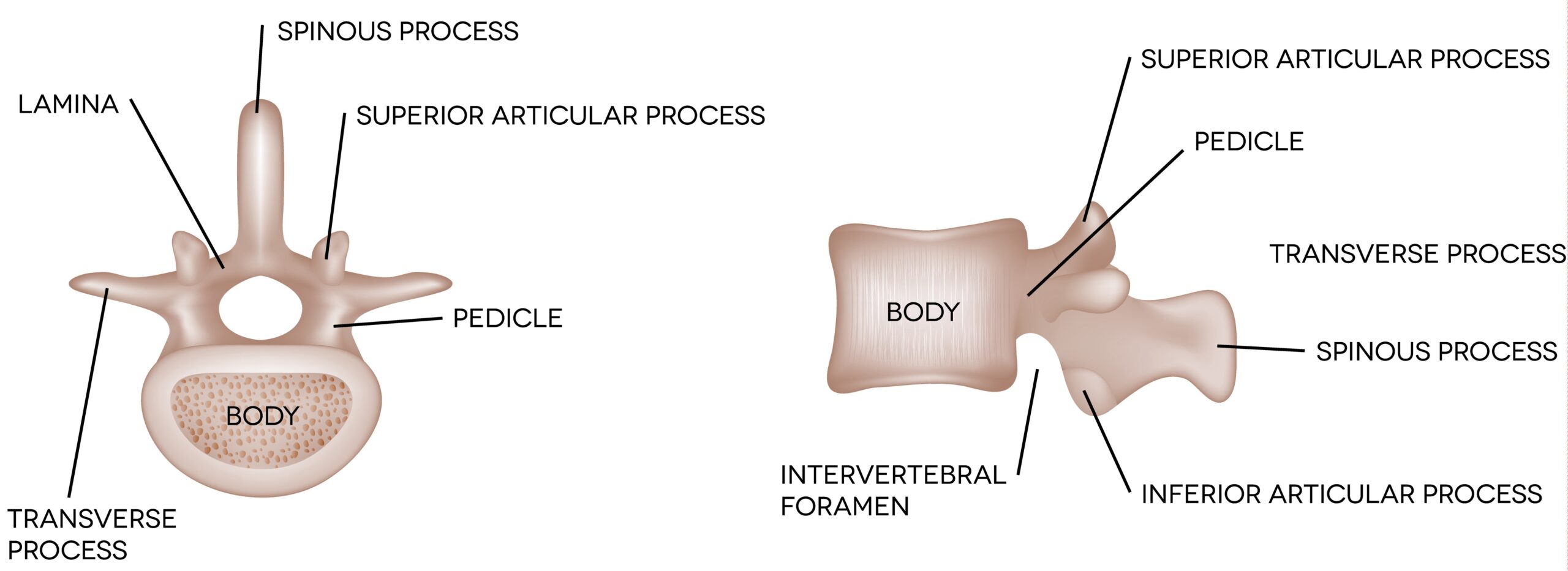
Each vertebra has two pedicles—one on the left and one on the right. The pedicles extend from the back of the vertebral body and connect to the posterior elements (including the lamina). If you picture a ring, the pedicles are the strong side pillars that help form the ring around the spinal cord (the spinal canal).
The term you’ll also see is “pedicle of the vertebrae”—that’s the same structure. When clinicians talk about a “spine pedicle,” they are usually referencing this bony segment as a landmark for imaging or procedures.
Pedicle anatomy and function
Where the pedicles sits
- Anterior: Vertebral body (weight-bearing block)
- Posterior: Lamina and posterior elements (protective/structural components)
- Medial: Spinal canal (spinal cord or cauda equina)
- Lateral: Foramina (nerve exit zones)
What the pedicles do
- Stability: A core load-transfer connection between the front and back of the vertebra.
- Protection: Helps form the protective ring around neural elements.
- Nerve pathways: Defines parts of the foramina—critical real estate for nerve roots.
- Procedural landmark: Important for safe needle trajectories and for surgical instrumentation.
How pedicles differ by spinal region
Pedicles change size and orientation depending on the region, reflecting different mechanical demands and motion patterns:
Cervical spine (C1–C7)
- Smaller pedicles, designed for mobility.
- Clinical relevance: careful planning is essential for any instrumentation due to smaller dimensions.
Thoracic spine (T1–T12)
- More rigid region (rib cage support), pedicles tend to angle differently.
- Clinical relevance: fractures, tumors, and deformity workups often rely on CT detail.
Lumbar spine (L1–L5)
- Larger, stronger pedicles—built for load-bearing and motion.
- Clinical relevance: many common back/leg pain syndromes relate to the lumbar foramina and nerve roots.
Why pedicles matters (pain, nerves, and procedures)
These amazing bony bridges matters because it sits at the crossroads of stability and nerve pathways. When something affects the pedicle (fracture, tumor, stress reaction, degenerative narrowing), the nearby nerve roots and spinal canal can be impacted—leading to symptoms like back pain, sciatica, numbness, or weakness.
Why the pedicles Are the gateway to vertebral-body procedures
Clinically, the spinal pedicle matters because it sits next to the spinal canal and helps define the nerve exit zones (foramina). It’s also a reliable bony landmark that physicians and surgeons use with imaging guidance to safely navigate to the vertebral body during minimally invasive procedures.
Procedures that access the vertebral body
- Kyphoplasty (compression fractures): a balloon is used to create space, then cement stabilizes the fractured
vertebra to reduce pain and limit collapse. - Vertebroplasty (compression fractures): bone cement is injected into a painful vertebral fracture to strengthen the bone and improve stability.
- Intracept® (basivertebral nerve ablation): a minimally invasive approach that targets the basivertebral nerve inside the vertebral body for certain types of chronic vertebrogenic low back pain.
sensitive structures (spinal cord/nerve roots) while reaching the vertebra with precision.
Common pedicle-related conditions
1) Stress or Traumatic Fractures Involving the Pedicle
A pedicle fracture can occur after a fall, accident, or repetitive load (stress injury). Symptoms often include localized pain that worsens with movement; in some cases, instability or nerve irritation can develop.
2) Degenerative foraminal narrowing (nerve compression zone)
Although discs and facet joints often get the spotlight, foraminal narrowing can also relate to bony boundaries near the pedicle. When the foramen tightens, nerve roots may be irritated—causing radiating pain, tingling, or weakness.
3) Pedicular sclerosis / stress reaction
“Sclerosis” on imaging can reflect chronic stress, degenerative change, or other processes. The key is correlating imaging with symptoms and ruling out concerning causes when appropriate.
4) Tumor or metastatic involvement
The spine is a common location for metastatic disease. When the pedicles are involved, it can increase fracture risk or cause pain. This is one reason clinicians take persistent night pain, unexplained weight loss, and history of cancer seriously.
5) Infection (less common but important)
Spinal infections can involve bone. Fever, immune compromise, IV drug use, recent infection, or elevated inflammatory markers raise concern—prompt evaluation matters.
Diagnosis and imaging: X-ray vs CT vs MRI
Clinical evaluation
A focused exam looks for pain patterns (mechanical vs inflammatory), neurologic deficits (strength, reflexes, sensation), and red flags. If symptoms suggest nerve involvement, imaging and targeted testing may be appropriate.
Imaging choices
- X-rays: Good first look for alignment, obvious fracture, and degenerative change.
- CT: Best for detailed bony anatomy—excellent for pedicle fractures or complex bone evaluation.
- MRI: Best for nerves, discs, marrow changes, tumor/infection suspicion, and soft tissue.
- Bone scan / nuclear imaging: Useful in select cases for stress injury, cancer activity, or multifocal processes.
Treatment options
Treatment depends on the cause (fracture vs nerve compression vs tumor vs infection), severity, stability, and neurologic status.
Conservative care
- Activity modification: Protect the region while healing; avoid provocative loads.
- Medication: Anti-inflammatories (when appropriate) and pain control strategies.
- Physical therapy: Core stability, mobility, posture, and graded return to activity.
Interventional options (selected cases)
- Vertebroplasty / Kyphoplasty: For certain vertebral compression fractures to stabilize bone and reduce pain.
- Targeted injections: When nerve irritation is present, image-guided injections can be diagnostic and therapeutic.
- Radiofrequency ablation: In select pain generators (or oncology-related pain pathways), RFA may help.
- Oncology collaboration: If metastatic disease is present, treatment may include radiation, systemic therapy, and stabilization strategies.
Surgery / instrumentation
In cases of instability, severe fracture, progressive deformity, or neurologic compromise, surgical options may be considered. In that world, the pedicle is a critical anatomic corridor for stabilization (e.g., pedicle screws).
Red flags: seek urgent evaluation if you have
- New or progressive weakness, foot drop, or significant numbness
- Bowel/bladder changes or saddle anesthesia
- Fever, chills, or suspected infection
- History of cancer with new severe spine pain
- Severe trauma or pain that is rapidly worsening
FAQ
Is the pedicle a disc?
No—discs are soft tissue cushions between vertebral bodies. The pedicle is bone.
Can a “pedicle problem” cause sciatica?
It can, depending on how it affects the foramen and nearby nerve roots (often in the lumbar spine).
What test best shows a pedicle fracture?
CT is typically best for bone detail. MRI can add information about marrow injury and nearby soft tissues.
Next step if you’re unsure what your imaging means
If you have persistent back pain, radiating leg symptoms, or a recent injury, a targeted evaluation can clarify whether your symptoms match the imaging findings and what options make sense.
Dr. Amit Sharma & our minimally invasive pain & spine team.
External references (for deeper reading)
- Intervertebral foramen anatomy (formed between adjacent pedicles):
Kenhub - Pedicle screw insertion basics (surgical reference):
AO Foundation Surgery Reference - Intracept (basivertebral nerve ablation) overview:
Cleveland Clinic



