
Spondylolisthesis Definition: 5 Essential Nomenclature Rules
- Posted on: Dec 24 2025
Last reviewed: 2025-04-19 • Reviewed by Dr. Amit Sharma, MD
If you have read an MRI report that mentions spondylolisthesis, anterolisthesis, retrolisthesis, degenerative, isthmic, or Meyerding Grade I, you are not alone—this language can be confusing. The problem is not that the terms are “wrong.” It’s that they describe different parts of the same diagnosis, and they are often used without explaining what each piece means. This guide begins with a clear spondylolisthesis definition, then explains spondylolisthesis nomenclature so you can decode reports accurately.
What Is Spondylolisthesis? (Spondylolisthesis Definition)
Spondylolisthesis means that one vertebra has translated (slipped) relative to the vertebra below it. In the lumbar spine, spondylolisthesis can narrow the spinal canal or the neural foramina (the openings where nerves exit), contributing to back pain, leg pain, numbness, tingling, weakness, or walking intolerance—especially when stenosis is present. That is the core spondylolisthesis definition.
Importantly, “spondylolisthesis” is a descriptive diagnosis. The spondylolisthesis definition tells you a slip exists. It does not, by itself, tell you why the slip happened, which direction it occurred, or how severe it is. That extra detail is provided by spondylolisthesis nomenclature.
The Big Idea: Spondylolisthesis Nomenclature Is a “3-Part Diagnosis”
The most reliable way to avoid confusion is to treat spondylolisthesis nomenclature like a simple recipe with three independent parts:
- Cause / Type (WHY): what structural process created the slip (degenerative, isthmic, traumatic, etc.)
- Direction (WHICH WAY): anterolisthesis (forward) vs retrolisthesis/posterolisthesis (backward)
- Severity / Grade (HOW MUCH): often described using Meyerding Grade I–V or percent translation
Key point in spondylolisthesis nomenclature: Anterolisthesis/retrolisthesis are direction terms, not “types” of spondylolisthesis.
Rule #1: “Type” Means the Cause (WHY the Slip Happened)
In spondylolisthesis nomenclature, clinicians classify spondylolisthesis based on the underlying cause. The two most common types in everyday practice are:
- Degenerative spondylolisthesis — a wear-and-tear process involving disc degeneration, facet joint arthritis, and ligament laxity (often at L4–L5, typically later in life).
- Isthmic spondylolisthesis — a pars interarticularis defect (spondylolysis) that allows translation (often at L5–S1, frequently begins earlier in life).
Other categories include dysplastic (congenital), traumatic, pathologic, and iatrogenic causes. For the full overview, see: Spondylolisthesis (All Types).
- Degenerative spondylolisthesis — stenosis, neurogenic claudication, minimally invasive options
- Isthmic spondylolisthesis — pars defects, spondylolysis vs slip, athletic risk factors
Rule #2: “Direction” Means Forward vs Backward (WHICH WAY)
Direction is simple, but it is commonly misused as if it were a type. Good spondylolisthesis nomenclature separates direction from cause.
- Anterolisthesis = the upper vertebra has translated forward relative to the one below.
- Retrolisthesis (also called posterolisthesis) = the upper vertebra has translated backward relative to the one below.
Direction terms can occur with any type of spondylolisthesis. That’s why the spondylolisthesis definition alone is not enough—you need the full spondylolisthesis nomenclature.
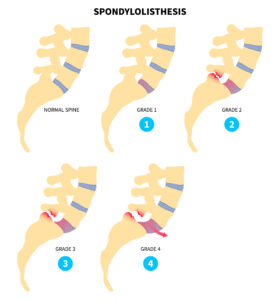
Rule #3: Meyerding Grading Defines HOW MUCH Slip Exists
Meyerding grading describes the amount of translation of one vertebra relative to the vertebra below it. Many radiologists report the percent slip, then group it into grades:
 |
|
What Meyerding grade does NOT tell you: it does not define the type (degenerative vs isthmic), it does not define direction (antero vs retro), and it does not guarantee symptom severity. Symptoms depend on stenosis, foraminal narrowing, nerve irritation, instability, and other factors—not just the grade.
Rule #4: Decode Any Report by Extracting the Three Labels
When you read imaging language, extract the three labels in order. This is the fastest way to apply the spondylolisthesis definition plus correct spondylolisthesis nomenclature:
- Type (WHY)
- Direction (WHICH WAY)
- Grade (HOW MUCH)
- “L4–5 Grade I anterolisthesis with facet arthropathy and stenosis” → Degenerative + Anterolisthesis + Grade I
- “L5–S1 pars defects with Grade II anterolisthesis” → Isthmic + Anterolisthesis + Grade II
- “Retrolisthesis at L3–4” → Direction is given, but type and grade may require context (disc/facet wear, % slip, stability)
Rule #5: Use the “Complete Sentence” Format (Unambiguous)
The most precise way to communicate the diagnosis is to use all three labels in one sentence. This makes the spondylolisthesis definition complete and makes spondylolisthesis nomenclature unambiguous:
- Degenerative spondylolisthesis with Grade I anterolisthesis at L4–L5
- Degenerative spondylolisthesis with retrolisthesis at L3–L4 (add grade/% if reported)
- Isthmic spondylolisthesis with Grade II anterolisthesis at L5–S1
If you only remember one thing, remember this:
Type answers WHY, direction answers WHICH WAY, and Meyerding grade answers HOW MUCH.
Where to Learn More (and What to Read Next)
- Spondylolisthesis (All Types) — overview, symptoms, diagnosis, and stepwise treatment options
- Degenerative spondylolisthesis — stenosis, walking intolerance, minimally invasive options
- Isthmic spondylolisthesis — pars defects, spondylolysis vs slip, athlete patterns
For more national education on spondylolisthesis definition and classification, see:
AAOS: spondylolysis and spondylolisthesis.
Dr. Amit Sharma & our minimally invasive pain & spine team.
If your MRI or X-ray report mentions spondylolisthesis, anterolisthesis, retrolisthesis, or a Meyerding grade, consider scheduling a consultation. A focused, minimally invasive evaluation can help identify the true pain source and build a personalized treatment plan.
For broader education from major medical organizations, you can also review:
AAOS overview of adult spondylolisthesis,
Cleveland Clinic’s spondylolisthesis explanation,
and Mayo Clinic’s spondylolisthesis guide.
Tagged with: Back Pain, Sciatica, spondylolisthesis
Posted in: Special Report, News



