
Why Does Kyphoplasty Relieve Pain So Fast? The Science Behind Rapid Pain Relief After Vertebral Compression Fractures.
- Posted on: Jun 2 2026
The Leading Hypotheses
Several mechanisms have been proposed, and more than one is likely operative in any given case. They are not mutually exclusive, but they are not equally supported by evidence either.
Mechanical Stabilization
This is the dominant early mechanism, and the one with the strongest convergent support across the literature. Although not perfectly established, the most likely mechanism for pain relief after kyphoplasty, even without significant restoration of vertebral body height, appears to be mechanical stabilization of the vertebral body.A
Vertebral compression fractures are painful in large part because of micromotion at the fracture site. Repetitive loading across unstable fragments continuously stimulates nociceptors in periosteal and trabecular bone. Both vertebroplasty and kyphoplasty increase spine segment stiffness from the fractured state, and pain reduction may be due to reduced micromotion between bone fragments.B
Cement eliminates that micromotion upon polymerization. The nociceptive stimulus is removed mechanically. This explains the rapid onset without requiring any thermal or neurochemical mechanism. It also explains why even late-intervention kyphoplasty, performed weeks after fracture, can still produce significant pain relief. Patients undergoing later intervention have been observed to experience significant improvement in pain scores following the procedure, likely in part due to the stabilizing and load-sharing effect of the cement in the setting of an unhealed vertebral body fracture with persistent micromotion.C
Basivertebral Nerve Thermal Modulation
The basivertebral nerve, or BVN, originates from the sinuvertebral nerve and enters the vertebral body through the basivertebral foramen, arborizing within the vertebral body and endplates. Histologic and clinical studies have demonstrated that the BVN is an important nociceptive pathway in vertebrogenic pain.D,E
It has become a specific target of interest through multiple prospective clinical trials, including the SMART and INTRACEPT studies, which demonstrated significant and durable improvements in pain and function following dedicated intraosseous radiofrequency ablation of the BVN in appropriately selected patients with vertebrogenic pain associated with Modic changes.E,F
The hypothesis as applied to kyphoplasty is that cement polymerization may generate sufficient localized heat to injure or partially denervate intraosseous nociceptive fibers, including branches of the BVN. Whether temperatures consistently reach neuroablative thresholds in vivo remains uncertain and likely depends on cement volume, cement geometry, and local tissue characteristics.
This is not implausible: peak PMMA cement temperatures ranging from 44°C to 113°C have been noted in cadaveric and experimental models, and this has been hypothesized to contribute to pain relief through the exothermic reaction of polymerization.G A landmark in-vitro study by Deramond et al. specifically hypothesized that temperatures generated during vertebroplasty cement polymerization may be sufficient to cause thermal necrosis of intravertebral neural tissue.H
Importantly, measured temperatures vary substantially depending on location. While temperatures adjacent to the cement bolus may exceed thresholds associated with neural injury, temperatures farther from the cement mass decline rapidly. As a result, demonstrating heat generation is not the same as demonstrating reproducible BVN ablation in clinical practice.
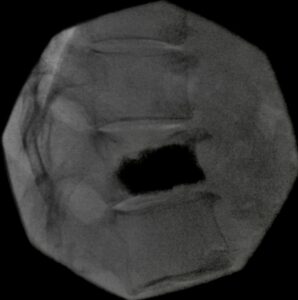
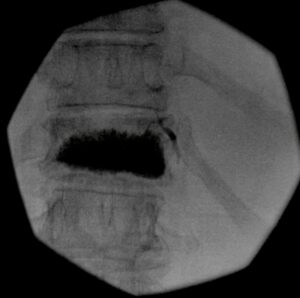
I want to be direct about something here: whether cement actually reaches the posterior vertebral body, through which the BVN enters and where many of its intraosseous branches course, depends heavily on technique and on how deliberately the operator pursues that goal. In my practice, posterior body cement distribution is an explicit intraoperative objective, not an afterthought. The fluoroscopy sequence below, a real T12 kyphoplasty case using a unipedicular Stryker approach, shows what intentional posterior fill looks like progressing through the procedure from cannula placement through final fill.
 |
 |
 |
The honest qualification that follows is this: even with posterior body reach, the thermal dose delivered to the BVN depends on cement bolus geometry, distance from BVN branches, cement volume, and where the exotherm curve peaks during polymerization. Geometric proximity is necessary but not sufficient to confirm BVN ablation as a reproducible mechanism in kyphoplasty specifically. The INTRACEPT and SMART data are compelling for dedicated RF ablation. Extrapolating that concept to cement exotherm, while scientifically plausible, remains a hypothesis rather than established proof.
Periosteal Decompression
Balloon inflation and height restoration may transiently decompress periosteal nerve endings under load. This is speculative as a standalone mechanism, but likely contributes to the early intraoperative and immediate post-procedure experience in cases where meaningful height restoration is achieved.
Procedural Context and the Sham Trial Problem
Intellectual honesty requires acknowledging the most uncomfortable data in this field. In 2009, two randomized sham-controlled trials published simultaneously in the New England Journal of Medicine, Kallmes et al. and Buchbinder et al., found that vertebroplasty produced similar improvements to a sham procedure at one to three months.I,J
Both trials generated immediate and lasting controversy. Critics pointed out that the cement volumes used were below what many experienced operators would consider therapeutic, that patient selection criteria excluded many of the most severely affected patients typically treated in practice, and that the sham injection itself, local anesthetic to the periosteum, may have had an active analgesic effect rather than serving as a true inert control.K
The trials have not settled the debate, and the broader literature, including multiple prospective registry studies and the FREE randomized trial comparing kyphoplasty to non-surgical management, continues to support the efficacy of augmentation in appropriately selected patients. But the sham data cannot be fully dismissed, and it appropriately keeps the field honest about the limits of what we can attribute to any specific mechanism.
At the same time, subsequent randomized studies, large registry analyses, and meta-analyses have generally supported vertebral augmentation in carefully selected patients with symptomatic acute fractures. The modern debate is less about whether augmentation can work and more about which patients derive the greatest benefit and through which mechanisms that benefit occurs.
What RF-TVA Adds to This Conversation
The RF-TVA platform, including the StabiliT system, which I have also used, is worth noting here because it introduces radiofrequency energy directly into the cement delivery process, controlling viscosity while potentially contributing thermal effect beyond passive cement exotherm.
Published biomechanical work comparing RF-TVA to balloon kyphoplasty shows that the approach achieves significantly greater trabecular interdigitation, 66.5% versus 16.7%, which has both structural and potentially neurochemical implications.L Whether greater cement interdigitation translates into a clinically meaningful difference in neural modulation, pain reduction, or BVN-related effects has not been directly evaluated in comparative mechanistic studies. It remains a plausible hypothesis awaiting direct investigation.
What We Can Say With Confidence
Kyphoplasty often works quickly and predictably in appropriately selected acute and subacute osteoporotic vertebral compression fractures. Mechanical stabilization is well-supported and explains the early timeline convincingly. BVN thermal modulation is a compelling secondary hypothesis, particularly when the operator achieves intentional posterior body cement distribution, but remains incompletely proven in the kyphoplasty-specific context.
The most likely reality is that kyphoplasty is not a single-mechanism therapy. Mechanical stabilization, altered load distribution, local neural modulation, and fracture healing likely contribute in varying proportions depending on fracture morphology, timing, cement distribution, and individual patient biology.
The full mechanistic picture is not settled science, and acknowledging that is part of what distinguishes a physician-authored account from a manufacturer brochure.
The best outcome metric isn’t which mechanism you believe. It’s whether your patient calls the next morning and tells you they slept through the night for the first time in three weeks.
References
- Staribacher A, et al. The outcome of radiofrequency kyphoplasty in the treatment of vertebral compression fractures in osteoporotic patients. J Clin Med. 2019;8(5):611. PMC6547388.
- Wilson DR, et al. An ex vivo biomechanical comparison of a novel vertebral compression fracture treatment system to kyphoplasty. Clin Biomech. 2012;27(2):128–135.
- Khan MA, et al. The effect of time to balloon kyphoplasty on osteoporotic vertebral compression fractures: a systematic review with meta-analysis. NASSJ. 2024. doi:10.1016/j.xnsj.2024.100269.
- Antonacci MD, Mody DR, Heggeness MH. Innervation of the human vertebral body. Spine. 1998.
- Fischgrund JS, et al. Intraosseous basivertebral nerve ablation for chronic low back pain: 2-year results from a prospective randomized double-blind sham-controlled multicenter study. Int J Spine Surg. 2019.
- Smuck M, Khalil J, Barrette K, et al. Prospective, randomized, multicenter study of intraosseous basivertebral nerve ablation for the treatment of chronic low back pain: 12-month results. Reg Anesth Pain Med. 2021;46(8):683–693. doi:10.1136/rapm-2020-102259.
- Deramond H, et al. Temperature measurement during polymerization of polymethylmethacrylate cement used for vertebroplasty. Spine. 1999.
- Deramond H, et al. Temperature elevation caused by bone cement polymerization during vertebroplasty. Bone. 1999;25(2 Suppl):17S–21S.
- Kallmes DF, Comstock BA, Heagerty PJ, et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med. 2009;361(6):569–579. doi:10.1056/NEJMoa0900563.
- Buchbinder R, Osborne RH, Ebeling PR, et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med. 2009;361(6):557–568. doi:10.1056/NEJMoa0900429.
- Clark W, et al. Randomized vertebroplasty trials: bad news or sham news? AJNR Am J Neuroradiol. 2009;30(10):1808–1809. PMC7051274.
- Krüger A, et al. Cement interdigitation and bone-cement interface after augmenting fractured vertebrae: a cadaveric study. Int J Spine Surg. 2012;6:115–121. PMC4300889.
Posted in: Special Report



